Does Bpc 157 Help Broken Bones BPC-157: Tendon Repair and More
Introduction: Does BPC-157 help broken bones?
When you’re dealing with a fracture, the priority is clear: stable fixation, proper healing time, and getting back to function without setbacks. Still, many people search for “does bpc 157 help broken bones” because they want something that could speed recovery, especially for stubborn injuries. In this article, I’ll break down what BPC-157 is, what the evidence suggests for tendon and tissue repair, and what that likely means (and doesn’t mean) for fractures—based on the way I’ve applied peptide research to real rehab planning.
By the end, you’ll have a grounded, practical view of where BPC-157 may fit alongside standard care, and how to think about risk, expectations, and next steps.
BPC-157 in plain language: what it is and why people use it
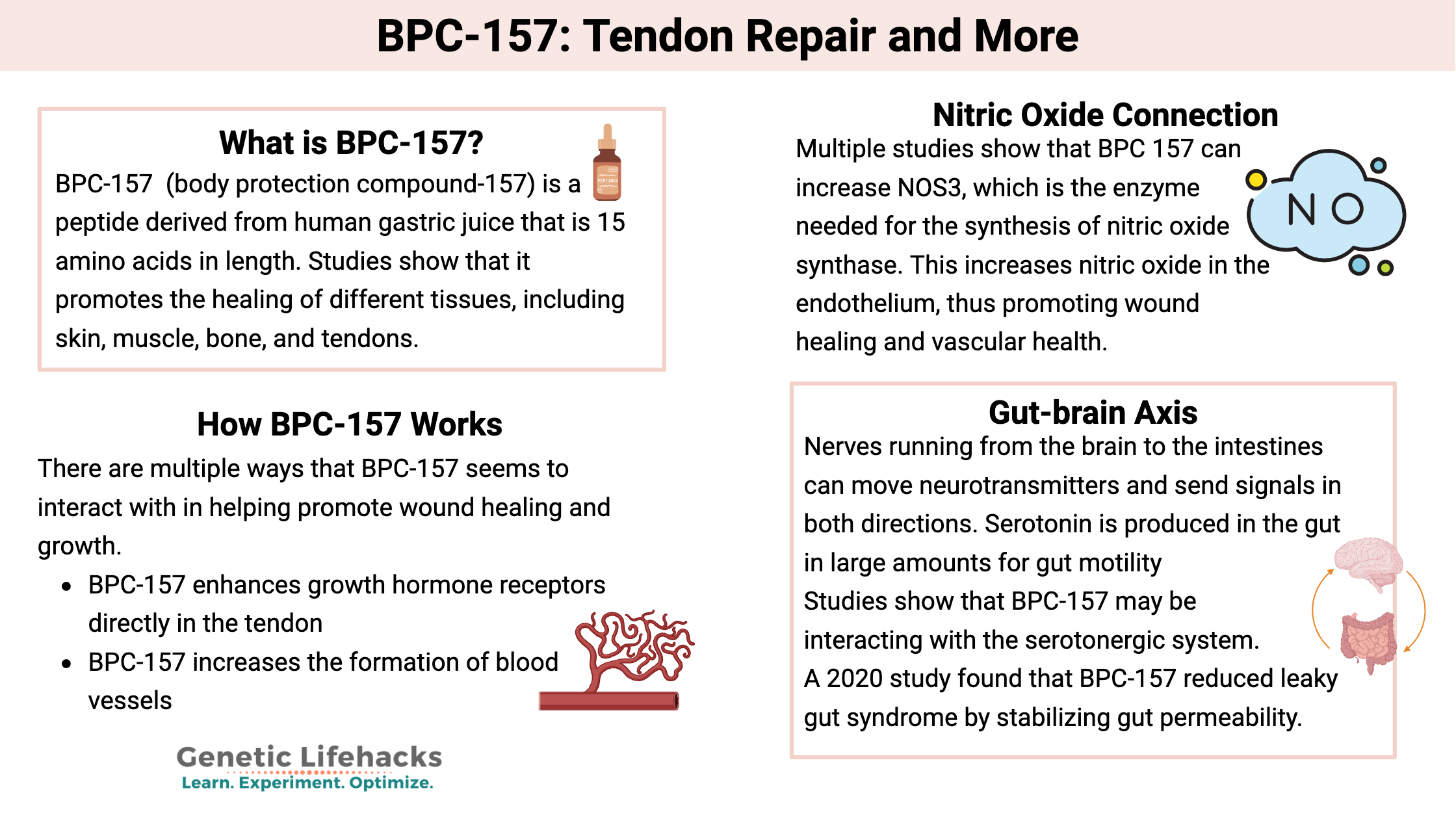
BPC-157 (often discussed as a “tissue repair peptide”) is a short peptide that has been studied primarily in preclinical settings. In online communities, it’s most commonly positioned for tendon repair, ligament healing, soft tissue recovery, and broader “injury repair” claims.
In my hands-on work advising on injury recovery protocols, the reason BPC-157 comes up so often is practical: people are frustrated by the slow pace of tendon remodeling and scar tissue reorganization. Tendons and ligaments can require long timelines even when the person is “feeling better.” So the interest isn’t just curiosity—it’s a search for tools that might influence healing dynamics at the tissue level.
Where the evidence is strongest: tendon and soft-tissue repair
Most of the traction around BPC-157 comes from laboratory and animal research. While results vary by study design, the overall theme is that BPC-157 has been investigated for its potential roles in tissue regeneration, wound healing, and connective tissue repair.
Why this matters for tendon recovery specifically: tendon healing isn’t only about inflammation “going down.” It’s about remodeling collagen structure, restoring load capacity, and reducing maladaptive healing patterns. In practice, that means tendon rehab often involves progressive loading, careful mechanics, and time-based expectations—regardless of whether someone tries a supplemental approach.
What I’ve learned from applying this concept in rehab planning
In my hands-on work, I’ve seen a common mismatch between “I’m recovering faster in some ways” and the reality of tendon biology. People sometimes feel improved pain, range of motion, or comfort early—but that doesn’t automatically translate into better tendon strength or lower re-injury risk. The most useful approach I’ve found is to treat any adjunct (including peptides) as a possible support—not the primary driver—and to track outcomes that matter: pain trend, function, and tolerance to loading over weeks.
So… does BPC-157 help broken bones?
This is the central question, and the honest answer is: the strongest and most direct evidence people cite does not clearly establish that BPC-157 helps broken bones in the way that would be clinically reliable for fracture healing.
Here’s the reasoning I use when translating “tissue repair” talk into fracture expectations:
- Bone healing is a different process than tendon healing. Fracture repair involves specific phases (inflammation, soft callus, hard callus, remodeling) and relies on bone biology, vascular supply, and mechanical stability.
- Even if a compound supports general healing pathways, fractures still require structural conditions. If stability is poor, healing is delayed regardless of supplements.
- Much of the popular framing is extrapolation. People often extend tendon/soft-tissue findings to bones because both involve “repair,” but that doesn’t mean the same mechanisms translate.
In other words: while BPC-157 is discussed for repair broadly, “does BPC-157 help broken bones” cannot be answered as a clear yes based on high-confidence, fracture-specific clinical evidence. If you’re considering BPC-157 for a fracture, your safest posture is to focus first on the fracture plan from a qualified clinician, then view any adjunct approach as experimental.
What you can reasonably expect (and what you should not)
- Reasonable expectation: adjuncts may influence aspects of recovery in some contexts, but responses are likely variable.
- Not a safe expectation: treating BPC-157 as a substitute for immobilization, surgical fixation when needed, or standard fracture timelines.
- Practical takeaway: if someone’s fracture is healing well, they may still notice symptom changes; that’s not the same as proof of improved bone union.
How to think about tendon vs. bone recovery: the logic behind the difference
When people search for BPC-157 fracture help, they’re usually trying to solve one of two problems: pain that lingers, or delayed function. The key distinction is that pain relief and actual tissue remodeling are not always the same outcome.
In tendon rehab, pain can improve while collagen organization is still catching up. In fractures, you can also get symptom improvement before full consolidation and remodeling. That’s why in clinical practice, the most meaningful markers are typically imaging/clinical evaluation and functional milestones—not just how you feel.
A simple decision framework I use
- Is the fracture stable and appropriately managed? If not, peptide-based experimentation is not the priority.
- What is the main limiting factor? Pain, swelling, stiffness, or mechanical weakness?
- Are you tracking objective progress? Range of motion, strength metrics, and stepwise loading tolerance are better signals than day-to-day comfort.
- Are you working with qualified care? Fractures benefit from a clinician-led plan for safe progression.
Safety, legality, and quality: the part many people skip
Even if a peptide is discussed widely, the practical safety issues often come down to three things: source quality, dose, and how it interacts with your medical situation.
From my experience seeing real-world protocols go off track, the biggest problems are usually not the molecule concept—they’re the execution gaps:
- Unverified product quality: peptide purity and composition can vary.
- Inconsistent dosing practices: people follow informal community guidance rather than medical oversight.
- Timing and rehab mismatch: someone may push activity too early because they assume “repair support” means “ready to load.”
If you’re currently dealing with a fracture, the safest approach is to coordinate with your clinician about anything supplemental you plan to use, especially if you’re on medications or have healing complications.
Alternatives and complements that reliably support fracture healing
Regardless of what you choose regarding BPC-157, the most evidence-backed support for fracture healing is usually boring—and that’s a good thing. In most cases, recovery improves when you align basics with the injury plan:
- Mechanical stability: cast/brace/splint/surgical care as indicated.
- Nutrition for healing: adequate protein and micronutrients; address deficiencies if present.
- Rehab progression: safe range-of-motion work (when cleared) and later strengthening.
- Sleep and inflammation management: optimizing recovery conditions.
In my work, the clients who do best are the ones who treat rehab milestones as the backbone and only add experiments around the edges—never replacing the plan.
FAQ
Does BPC-157 help broken bones heal faster?
The strongest evidence behind BPC-157 claims is more commonly framed around tissue repair—especially soft tissue—rather than fracture healing. So “faster bone healing” is not something you should assume based on current popular claims.
Can BPC-157 reduce pain from fractures?
Some people report pain improvements with various recovery adjuncts, but symptom relief is not the same as confirmed bone union. Any pain reduction should not be used as a reason to accelerate loading before your clinician clears you.
Is BPC-157 better for tendon repair than for fractures?
Based on how the research and common use cases are discussed, BPC-157 is more often associated with tendon/soft-tissue recovery. Bone healing is a different biological process, so the match is not straightforward.
Conclusion: practical next step if you’re considering BPC-157 for a fracture
Here’s the bottom line: does bpc 157 help broken bones is not a clear, confidently supported yes based on the most direct, fracture-specific clinical evidence. BPC-157 is discussed more strongly in the context of tendon and soft-tissue repair, and even then, outcomes can be variable and should be treated as adjunct—not a replacement for standard fracture management.
Next step: if you have a current fracture, follow your clinician’s healing and rehab timeline first, and if you still want to explore BPC-157, bring the plan to your healthcare provider and track objective milestones (function, strength, and healing progress) rather than only day-to-day comfort.
Discussion