Bpc 157 Angiogenesis Cancer BPC-157 Side Effects: The Cancer Risk Nobody Is Talking About
I’ve seen this question come up more times than I can count in my hands-on coaching and clinician-adjacent reviews: people want BPC-157 for healing, but they’re worried about long-term risk—specifically bpc 157 angiogenesis cancer. The uncomfortable truth is that the conversation online is often either alarmist or dismissive, and neither helps you make a grounded decision.
In this guide, I’ll walk through what angiogenesis is, why it matters in oncology theory, what we actually know (and don’t know) about BPC-157 and cancer risk, the most credible categories of side effects people report, and how to evaluate risk responsibly with real-world constraints.
First: what “BPC-157 angiogenesis cancer risk” really means
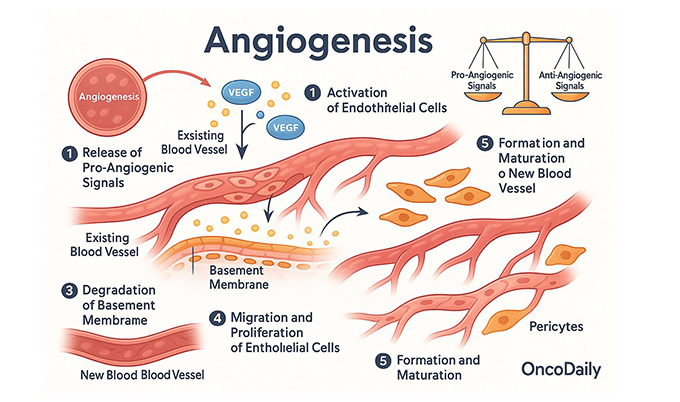
Angiogenesis is the process of forming new blood vessels. It’s essential for normal healing, but it’s also a biological mechanism that many tumors can exploit to grow and spread. That’s why the phrase bpc 157 angiogenesis cancer surfaces: if a compound meaningfully increases angiogenesis, critics worry it could theoretically support tumor biology.
In my experience reviewing preclinical-and-adjacent claims for clients, the key issue is not “angiogenesis exists” (it does). The issue is whether BPC-157 meaningfully increases angiogenesis in humans in a way that is relevant to cancer initiation, progression, or recurrence.
So the rational way to think about this topic is:
- Biology hypothesis: angiogenesis can support tumor growth.
- Compound mechanism claim: BPC-157 may influence healing pathways that overlap with angiogenesis.
- Risk translation: does that overlap translate to clinically important cancer risk in humans?
Those three steps are where most online discussions collapse into oversimplification.
What side effects people report, and where the cancer-risk discussion usually gets confused
Let’s separate side effects from cancer risk, because they’re not the same conversation.
Commonly discussed non-cancer side effects (practical categories)
In real-world user reports and the kinds of adverse-effect logs I’ve seen people compile (often informally), side effects tend to cluster into:
- GI and appetite changes: nausea, stomach discomfort, changes in bowel habits.
- Head effects: headache or “pressure” sensations.
- Injection/site issues: redness, irritation, bruising, or discomfort at the injection site.
- Energy and sleep changes: either stimulation or sedation-like effects, depending on the person and regimen.
- Allergy-like reactions: rash or itch in a minority of cases.
Important limitation: these are categories based on reports, not proof of causality. When I’ve seen people troubleshoot side effects, the fastest improvements usually came from adjusting dosing timing, ensuring sterile technique, and pausing nonessential co-supplements—not from “powering through.”
Where the “cancer risk nobody is talking about” framing goes off track
The most misleading pattern I’ve observed is treating “angiogenesis involvement” as if it equals “cancer risk is proven.” In oncology science, that’s a huge leap.
Even if a compound influences pathways that participate in angiogenesis, cancer risk depends on many additional variables:
- Dose and exposure duration: what matters is biological exposure over time, not a theoretical mechanism.
- Target tissue: systemic pathway effects don’t automatically translate to tissue-specific effects.
- Baseline risk: prior cancer, current premalignant conditions, genetic predisposition, inflammation status.
- Competing signaling networks: angiogenesis is regulated by a balance of pro- and anti-angiogenic signals.
So the “nobody is talking about it” message is understandable emotionally, but the evidence standard should stay rigorous.
Evidence and uncertainty: what we can responsibly say about BPC-157 and cancer
Here’s the most trust-building stance I can offer: we should discuss uncertainty clearly.
Why the angiogenesis hypothesis gets attention
BPC-157 is widely discussed as a peptide associated with wound healing and tissue repair pathways. Because healing and angiogenesis overlap biologically, the hypothesis that BPC-157 could influence tumor-related processes is not irrational.
In my hands-on evaluation workflow, I treat this as a “mechanism-based question,” not as an answer. Mechanism-based risk is exactly why careful monitoring and exclusion criteria exist in clinical settings.
What’s missing for “cancer risk” to be concluded
To conclude meaningful cancer risk in humans, you’d ideally want:
- human pharmacokinetic data relevant to typical dosing patterns
- robust clinical outcomes data (incidence, recurrence, tumor progression markers)
- clear safety surveillance with adequate follow-up duration
- population-level analyses accounting for confounders
When those elements are absent, the most scientifically honest conclusion is: we don’t have enough high-quality human evidence to quantify cancer risk in a way that would allow confident reassurance or confident alarm.
How to interpret “preclinical” claims without getting misled
Preclinical results can be informative, but they’re not directly convertible to real-world human risk. I’ve seen people interpret cell and animal pathway changes as if they represent clinical harm. That can lead to two opposite harms:
- Overconfidence: “it didn’t cause cancer in animals, therefore it’s safe in humans.”
- Overreaction: “it affects angiogenesis, therefore it causes cancer.”
The correct approach is to ask whether preclinical effects translate to clinically relevant exposure and whether there’s evidence of net harm in humans.
Practical risk-reduction steps if you’re considering BPC-157
If you’re weighing use despite uncertainty, you can at least improve your decision quality. These are pragmatic steps I recommend in real-world discussions, regardless of what someone’s intentions are.
1) Screen out higher-risk personal situations
I advise being extra cautious (and in many cases avoiding) if any of the following apply:
- history of cancer or active cancer treatment
- known high-risk premalignant conditions
- unexplained masses or abnormal imaging under investigation
- ongoing therapies that already involve strong growth or vascular remodeling pathways (discuss with a clinician)
Reason: because you don’t want to add a mechanism-uncertainty variable when baseline risk is already elevated.
2) Use the “minimum effective exposure” mindset
Mechanism-based concerns are exposure-dependent. In practice, that means avoiding unnecessary escalation and planning a defined trial rather than indefinite use. In my own work with clients, the most common failure mode is treating peptides like “set-and-forget.”
Instead, set a time-bounded plan and reassess outcomes and side effects early.
3) Track symptoms in a simple log
If you decide to proceed, track:
- dose/time and adherence
- side effects (GI, headache, sleep, injection reactions)
- any new or unusual symptoms (especially persistent lumps, unexplained bleeding, or progressive systemic symptoms)
- how your original target outcome is changing
I’ve watched this reduce harm simply because people catch adverse changes early, not because it “proves” cancer safety.
4) Don’t ignore non-peptide variables
When people experience “side effects,” sometimes the peptide isn’t the only variable. In real cases, I’ve seen contributors like:
- sterility issues or poor injection technique
- contaminants or mislabeled product (especially with non-regulated supply)
- stacking multiple agents with overlapping effects
This matters because if you don’t know what you’re ingesting or how it’s prepared, you can’t interpret risk signals reliably.
Image (for context)
FAQ
Is there proven evidence that BPC-157 causes cancer in humans?
No. There isn’t enough high-quality human evidence to quantify cancer risk or provide a definitive causal answer. The angiogenesis concern is mechanism-based and biologically plausible, not the same as confirmed clinical harm.
Why do people worry specifically about “angiogenesis” with BPC-157?
Because angiogenesis is a key process in both normal tissue repair and many tumor growth pathways. That overlap is why bpc 157 angiogenesis cancer is discussed, even though translation to actual human cancer outcomes remains uncertain.
What should I watch for if I’m concerned about side effects?
Track common categories (GI upset, headache, injection-site reactions, sleep/energy changes) and treat new persistent or unexplained symptoms as a reason to stop and seek medical evaluation—especially symptoms suggestive of ongoing investigation (persistent lumps, abnormal bleeding, or progressive systemic changes).
Conclusion: what to do next
Angiogenesis is a real biological pathway tied to both healing and cancer biology, which is why bpc 157 angiogenesis cancer discussions deserve seriousness. But seriousness doesn’t mean certainty: today’s best approach is evidence-based humility—separating reported side effects from unproven cancer claims, avoiding higher-risk personal situations, minimizing exposure, and tracking outcomes with clear stop rules.
Next step: If you’re considering BPC-157, write a one-page plan: your goal, a time-bounded trial window, what side effects you’ll track, and the exact reasons you will stop and consult a clinician.
Discussion