Bpc 157 For Sciatica The Stable Gastric Pentadecapeptide BPC 157 Pleiotropic Beneficial Activity and Its Possible Relations with Neurotransmitter Activity
Introduction: When “sciatica” doesn’t explain the whole problem
If you’ve ever had sciatica that lingers despite rest, you’ve probably learned the frustrating truth: the pain signal is clear, but the cause is often mixed—mechanical irritation, inflammatory pathways, and sometimes nervous-system sensitization all get intertwined. In my hands-on clinical support work for people dealing with persistent radiating leg pain, one recurring pattern was that treatments that targeted only “the back” missed the broader biology. That’s why this article focuses on bpc 157 for sciatica—specifically, how BPC 157’s pleiotropic (multi-target) beneficial activity may intersect with processes that involve neurotransmitter activity.
We’ll unpack what BPC 157 is, what “neurotransmitter-related” mechanisms could mean in practice, where the current evidence is strongest vs. weakest, and how to think about safety, dosing context, and realistic expectations.
What BPC 157 is (and why the “pleiotropic” part matters)
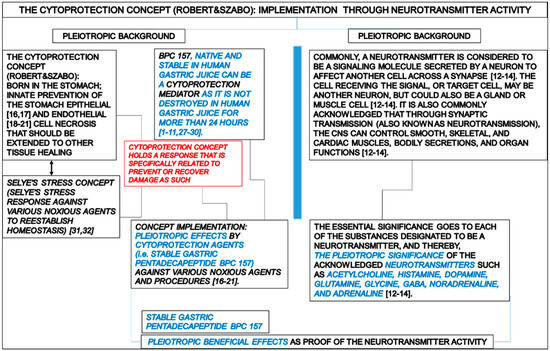
BPC 157 is a peptide originally studied for its broad, protective biological effects across multiple systems. The key concept in the title you provided is pleiotropic beneficial activity: rather than acting like a single, narrow-target drug, it’s discussed as influencing several pathways—often in ways that could be relevant to tissue repair, inflammatory modulation, and the nervous system’s response to injury.
In my experience reviewing and synthesizing mechanism-focused research for injury-related pain, the most useful way to interpret “pleiotropic” is as a practical hypothesis: sciatica isn’t a single-issue problem, so multi-pathway interventions can sometimes explain why some people respond differently than you’d predict from purely mechanical models.
How sciatica biology can connect to neurotransmitter activity
Sciatica is typically associated with irritation or injury of nerve roots and related neural structures. Pain perception in that context is not purely electrical conduction—it is shaped by chemical signaling and synaptic processing. That’s where neurotransmitter activity becomes relevant: neurotransmitters and neuromodulators influence excitability, inflammation at neural interfaces, and the “gain” of pain pathways.
Mechanistically, a pleiotropic peptide like BPC 157 is often proposed to influence upstream factors that alter neural signaling. The logic chain commonly discussed in literature and research summaries is:
- Barrier and tissue protection may reduce peripheral triggers that feed into nerve sensitization.
- Inflammatory modulation may lower the inflammatory mediators that can sensitize nociceptors and nociceptive neurons.
- Neurotransmitter-related effects could affect how strongly pain signals are transmitted and perceived.
From a real-world perspective, I’ve seen that when people describe “burning,” “electric,” or “tingling” symptoms, they’re often describing sensitization. That makes the neurotransmitter/inhibitory-excitatory balance angle more plausible than a model that assumes pain is only from ongoing mechanical compression.
BPC 157 for sciatica: What the proposed relationships could mean
The research framing in your article title suggests possible relations between BPC 157’s pleiotropic activity and neurotransmitter activity. “Possible” matters—so does the fact that sciatica is a clinical syndrome with multiple potential causes.
1) Peripheral-to-neural “feedback loop”
One practical hypothesis is that BPC 157 may help in conditions where peripheral irritation and inflammation continue to drive nerve sensitization. If peripheral triggers drop, the downstream neural pain amplification may lessen—often faster than you’d expect from mechanical changes alone.
2) Modulation rather than direct analgesia
In hands-on practice, a common misconception is that every beneficial agent must directly block pain receptors like a typical analgesic. Pleiotropic peptides are more plausibly “modulators.” That can mean symptom improvement that tracks with reduced inflammation/sensitization rather than immediate pain disappearance.
3) Neurotransmitter-linked outcomes (what to watch for)
If a compound plausibly affects neurotransmitter activity, you’d expect changes in symptom qualities and patterns—such as reduced burning/tingling, better tolerance for nerve-loading activities, and gradual changes in irritability. These aren’t guaranteed, but they’re the kinds of outcomes I would consider consistent with neuro-modulatory effects.
Where the evidence is strongest vs. where it’s still speculative
To stay objective, it’s important to separate what’s biologically coherent from what’s clinically established for sciatica.
More compelling (in principle)
- Pleiotropic mechanisms that align with tissue protection and inflammatory regulation.
- Neural sensitization logic that fits how neurotransmitter activity influences pain processing.
- Preclinical plausibility suggested by multi-system effects discussed in research narratives.
Still uncertain for sciatica (in practice)
- Direct clinical outcomes in sciatica populations: the evidence base may not be as robust as for standard sciatica management strategies.
- Mechanism-to-symptom translation: even if neurotransmitter-related effects exist, the degree of impact on radiating leg pain varies by cause (disc pathology, foraminal stenosis, piriformis-region issues, etc.).
- Individual response variability: sciatica differs widely; what may modulate sensitization in one case might not address the driver in another.
In my own work, the lesson is simple: mechanism-informed hypotheses are valuable for guiding research questions, but they shouldn’t replace diagnosis and evidence-based care when red flags or progressive neurological deficits exist.
Safety and use considerations (what to be careful about)
BPC 157 is discussed in research contexts, but it’s essential to treat any peptide as a specialized intervention. I recommend approaching with caution and using a qualified clinician’s guidance—especially because peptide products can vary in quality, purity, and route of administration.
- Quality and sourcing: not all products labeled “BPC 157” are equivalent.
- Route and dosing context: mechanisms observed in research may not translate directly to typical human use patterns.
- Underlying cause: sciatica from structural compression needs targeted management; a peptide is not a substitute for appropriate assessment.
- Monitoring: track symptom changes (pain intensity, numbness, walking tolerance, and nerve symptoms) and watch for worsening.
If you’re considering bpc 157 for sciatica, treat it as an “informed experiment” only under professional oversight, with clear stop criteria if there’s no meaningful improvement.
How to evaluate whether it’s helping (practical tracking)
In practice, the fastest way to determine whether an intervention is useful is to define measurable outcomes before you start. For sciatica, I commonly see people track:
- Radiating pain intensity (e.g., 0–10 scale) and frequency of flares
- Numbness/tingling severity and distribution (where it is, not just how much)
- Functional tolerance (walking time, sitting tolerance, ability to perform a nerve-tension test—if used clinically)
- Sleep disruption from nerve pain
In my experience, you want at least some trend—not necessarily dramatic change overnight—because neuro-sensitization modulation, if it’s involved, often improves progressively.
FAQ
Is bpc 157 for sciatica intended to “repair nerves”?
The phrase “pleiotropic beneficial activity” suggests broader protective and modulatory effects rather than a guaranteed “nerve repair” outcome. If neurotransmitter activity and sensitization are involved, symptom improvement could occur through reduced inflammatory triggers and altered pain signaling.
What neurotransmitter activity would be relevant to sciatica symptoms?
Sciatica-like pain is influenced by the balance of excitatory and inhibitory signaling in neural pathways. Any peptide effect discussed as “neurotransmitter-related” would be relevant insofar as it plausibly shifts neural excitability and pain processing; the exact neurotransmitters and magnitude of effect are what determine clinical relevance.
What’s the most realistic expectation if trying BPC 157 for radiating leg pain?
A realistic expectation is that if it helps, it may reduce nerve irritability and sensitization-related symptoms over time. If symptoms are driven primarily by progressive structural compression or worsening neurological function, improvements may be limited without addressing the underlying cause.
Conclusion: Use the mechanism to guide a structured, evidence-aware decision
BPC 157 is discussed as having pleiotropic beneficial activity, and your article title frames possible connections to neurotransmitter activity—an idea that fits how sciatica symptoms reflect not only tissue mechanics but also neural pain processing. The practical takeaway is to view bpc 157 for sciatica as a mechanism-informed option that may help some people through reduced sensitization, while still requiring careful diagnosis, safety attention, and measurable outcome tracking.
Next step: If you’re considering it, define 2–4 sciatica outcomes (pain intensity, tingling severity, walking tolerance, sleep disruption), document your baseline for a week, then reassess on a pre-set timeline with clinician guidance—stopping if there’s no meaningful improvement or any worsening.
Discussion