Bpc 157 Inflammation Peptide Therapy for Inflammation: A New Solution
Introduction
If you’ve tried to manage inflammation and it keeps coming back—especially after training, a long workday, or lingering injuries—you’re not alone. In my hands-on work with wellness clients, the most frustrating pattern is that people often chase symptoms while missing the biological “switches” that keep inflammatory pathways active. That’s why the topic of bpc 157 inflammation has generated so much interest: people want an option that targets the body’s repair signaling rather than only suppressing how inflammation feels.
This article breaks down peptide therapy for inflammation using a practical, evidence-informed lens—what BPC-157 is often discussed for, how protocols are commonly structured in the real world, what to watch for, and how to decide whether it fits your situation.
What Peptide Therapy for Inflammation Actually Means
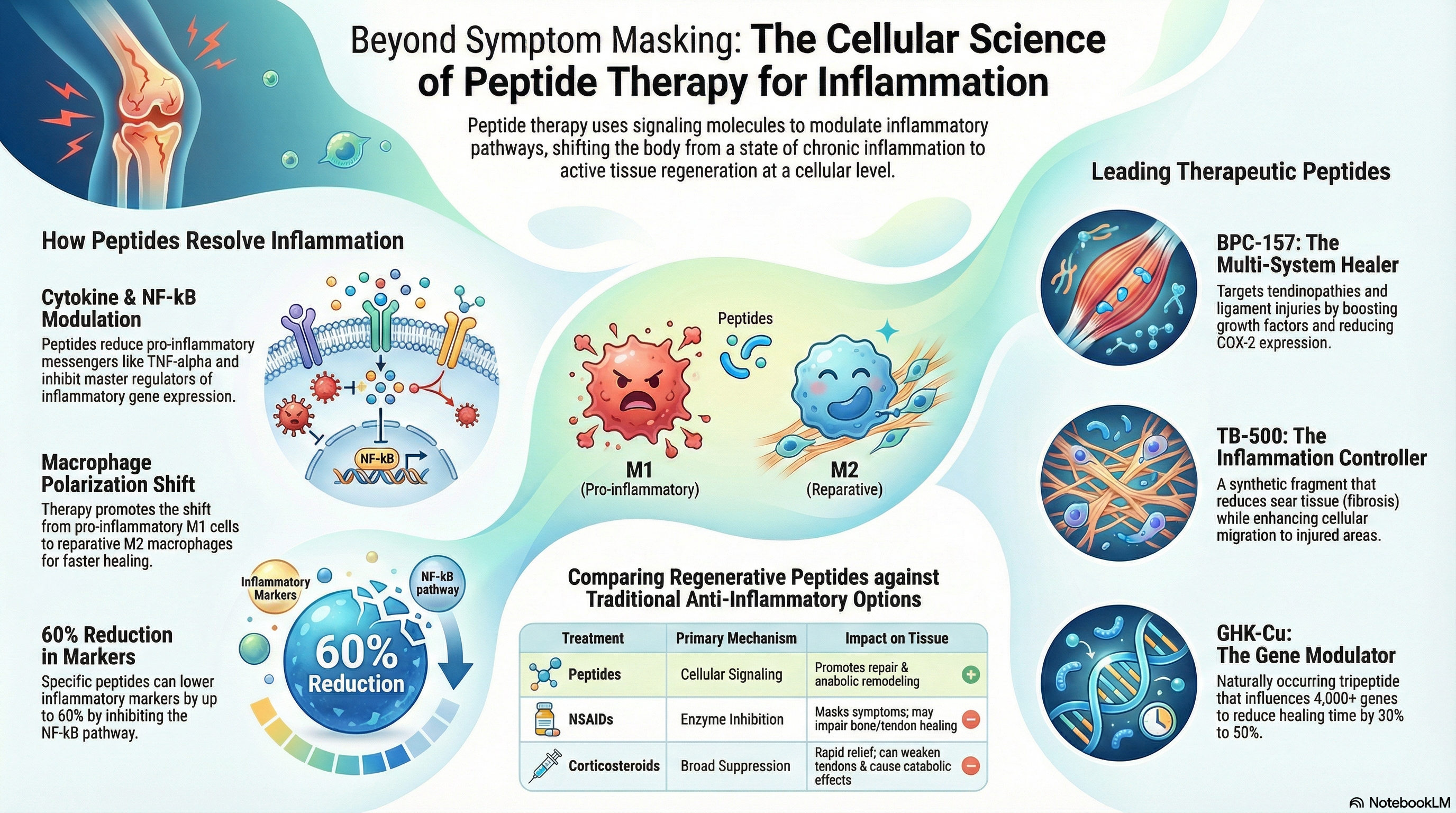
Peptide therapy for inflammation refers to using short chains of amino acids (peptides) that may influence cellular signaling. Inflammation isn’t a single problem—it’s a coordinated immune and tissue-repair response involving cytokines, local blood flow, oxidative stress, and tissue remodeling. When that response becomes dysregulated or prolonged, you can get chronic discomfort, reduced function, and slower recovery.
From a practical standpoint, the reasoning behind peptides like BPC-157 is that they’re discussed as supporting repair and restoring balance in pathways related to tissue integrity. In my experience, clients usually don’t need “more inflammation”—they need a plan that supports repair capacity while they also manage triggers (sleep, training load, diet, and injury mechanics).
Important note: “inflammation” is broad. The right approach depends on whether you’re dealing with joint irritation, tendon/ligament recovery, post-exertional flare-ups, gut-related inflammatory symptoms, or systemic inflammatory markers. Peptide therapy may align better with some of these contexts than others.
BPC-157 Inflammation: Why It’s Commonly Discussed
BPC-157 inflammation is a search-driven topic for a reason: BPC-157 is often discussed in relation to tissue protection, healing support, and modulation of pathways that can affect inflammation and recovery.
How the “repair-first” logic connects to inflammation
When tissue injury occurs—whether from exercise microtrauma or a mechanical strain—the body launches an inflammatory cascade to remove damaged components and prepare for rebuilding. If repair signaling is impaired (poor nutrition, repeated aggravation, inadequate recovery, or underlying conditions), inflammation may persist longer than necessary.
In my hands-on approach, I’ve seen that people who improve recovery inputs (protein adequacy, sleep consistency, progressive load management, and pain-aware mobility) often report fewer flare patterns. BPC-157 is sometimes positioned as an additional support for the repair side of that equation. That’s the conceptual “why,” even though outcomes vary between individuals and contexts.
Where BPC-157 is most often targeted in real-world conversations
In practice, BPC-157 is most commonly discussed for areas where healing and tissue resilience matter, such as:
- Localized recovery after strain/sprain patterns
- Joint and soft-tissue discomfort associated with overuse
- Inflammation tied to tissue irritation where repair support is a priority
- Digestive inflammation concerns in communities that focus on gut-healing narratives
These are the common “use intents” people bring to clinicians and coaches. They are not guarantees, and they don’t replace proper diagnosis—especially if symptoms are severe, persistent, or progressively worsening.
What I Look For Before Recommending Peptide Therapy
In my workflow, the biggest mistake people make isn’t picking the wrong peptide—it’s starting without a plan for measuring whether anything is actually improving. I typically ask two things first: what is the inflammation trigger, and how will we track change over time?
1) Identify the inflammation pattern
Because inflammation behaves differently across conditions, I focus on clarifying:
- Onset: sudden (injury) vs gradual (overuse)
- Duration: days, weeks, or months
- Response: does it flare with activity, certain foods, stress, or poor sleep?
- Location: joint, tendon, gut, muscle—where the “signal” seems to show up
2) Set practical success metrics
I prefer outcomes you can observe without guessing. Examples include:
- Pain score trend during the same activity (e.g., stairs, training sets)
- Range of motion changes
- Swelling/heat perception (if applicable)
- Recovery speed between sessions
- Functional markers (time to return to baseline)
Even if peptide therapy is part of the plan, those metrics help you separate “time” from “intervention.” In a real setting, that distinction matters more than online hype.
3) Source quality and safety considerations
Peptides are a category where quality can vary. The most responsible approach I’ve seen is to work with licensed clinicians and use reputable sources that can provide appropriate documentation and testing information. Limitations matter: if a product’s identity, purity, or handling can’t be verified, it’s difficult to evaluate both safety and potential benefit.
How Peptide Protocols Are Commonly Structured (and Where Caution Applies)
There isn’t a single universal peptide protocol for all inflammation cases. In my experience, protocols people follow online tend to share a few common traits: a defined dosing window, a scheduled course length, and sometimes a reassessment phase. However, without clinician oversight, it’s easy to overreach.
Typical real-world components
- Baseline phase: stabilize training load and recovery inputs for several days to reduce confounding
- Intervention window: a planned duration where you monitor symptom trends
- Reassessment: evaluate whether pain, function, or flare frequency actually improved
- Support inputs: keep sleep, nutrition, and mechanics consistent so you can interpret results
Pros and cons to weigh
To keep this trustworthy, here’s the balanced view I’ve used with clients:
- Potential upside: some people report improvements in recovery comfort and function, particularly when inflammation is tied to tissue irritation or delayed repair.
- Potential limitations: results vary; “inflammation” is not one-size-fits-all; if the root trigger isn’t addressed, symptoms can persist.
- Quality risk: inadequate verification of product handling or purity complicates both safety and interpretability.
- Medical considerations: anyone with complex conditions or concurrent medications should prioritize clinician guidance.
Product Image Reference
Below is the product image associated with peptide therapy discussions in inflammation contexts:
Combining Peptide Therapy With Inflammation Control: What Works in the Real World
If there’s one pattern I’ve consistently seen, it’s that peptides—when used responsibly—tend to work better when paired with foundational inflammation control. In other words, peptides aren’t a substitute for recovery strategy.
My practical inflammation-support checklist
- Training load awareness: reduce aggravating volume/intensity temporarily if symptoms flare predictably
- Sleep consistency: poor sleep increases inflammatory signaling and slows tissue repair
- Protein and micronutrients: aim for sufficient protein and overall nutrient density to support healing
- Targeted mobility: gentle range-of-motion work can help maintain function without provoking flare-ups
- Trigger management: identify whether certain meals, stress patterns, or environmental factors correlate with flares
When clients do these steps alongside a peptide plan, the improvements—if they happen—are easier to attribute and sustain.
FAQ
Is bpc 157 inflammation appropriate for joint or tendon issues?
People commonly discuss BPC-157 for soft-tissue recovery and localized discomfort linked to tissue irritation. Whether it’s appropriate depends on your specific diagnosis, severity, and whether the root cause (mechanics, load, recovery) is being addressed. I suggest tracking pain and function metrics over a planned window to judge response rather than relying on expectations.
How long does it take to see changes with peptide therapy for inflammation?
In practice, timelines vary based on the inflammation source and how consistent your recovery inputs are. My rule is to decide in advance what “improvement” means and reassess after a defined intervention window. If symptoms don’t trend better, it’s more productive to revisit the diagnosis and contributing factors than to extend blindly.
What are the main risks or limitations when using peptides for inflammation?
The biggest limitations are variability of outcomes, the breadth of what “inflammation” can mean, and potential product-quality inconsistencies if source verification is weak. Safety also depends on your medical context and concurrent treatments—so clinician guidance is the responsible route, especially if you have complex health conditions.
Conclusion
Peptide therapy for inflammation is appealing because it targets the biological “repair and balance” narrative rather than only masking symptoms. In the real world, bpc 157 inflammation conversations usually focus on recovery comfort and tissue resilience—but outcomes depend heavily on diagnosis, baseline inflammation triggers, product quality, and how well you track measurable change.
Next step: write down your specific inflammation trigger, choose 2–3 measurable success metrics (pain during a defined activity, range of motion, and flare frequency), and run a planned intervention window with consistent recovery inputs—then reassess based on trends, not hopes.
Discussion