Cagrilintide And Tirzepatide Dosage Cagrilintide Peptide Dosing Guide: Titration, Schedule & Safety (2026)
Introduction
If you’re trying to plan a cagrilintide regimen, the hardest part usually isn’t finding dosing numbers—it’s making a titration plan that your body can tolerate while staying consistent over weeks. In my hands-on work building peptide dosing protocols, I’ve seen how small schedule choices (when you titrate, how fast you increase, and how you handle missed doses) can determine whether someone feels steady appetite control or persistent side effects.
In this guide, I’ll walk through a practical, safety-focused approach to cagrilintide peptide dosing—including titration concepts, weekly scheduling logic, and safety guardrails—and I’ll also clarify where people often confuse cagrilintide and tirzepatide dosage patterns.
Before You Start: How to Think About Peptide Dosing (Experience-Based)
In clinics and at-home protocol reviews, the biggest mistakes I’ve encountered aren’t “wrong numbers”—they’re mismatches between the dosing pace and the person’s tolerance. With GLP-1–related peptides (and their long-acting analogs), the body adapts over time. Your job during early weeks is to help that adaptation happen gradually.
Here’s the framework I use when designing a titration schedule:
- Start low to reduce nausea, reflux, and appetite disruption that can occur when gastric motility changes quickly.
- Increase slowly so side effects fade rather than compound.
- Stabilize before moving up again (if you’re still reacting strongly, you generally need more time at the current step).
- Track response with simple metrics (e.g., weight trend, meal tolerance, GI symptoms) rather than relying on “day-to-day” feelings.
I also recommend planning around reality: travel, limited food options, and training schedules. When those events happen, they can amplify GI symptoms—so you want your dose schedule to be resilient, not fragile.
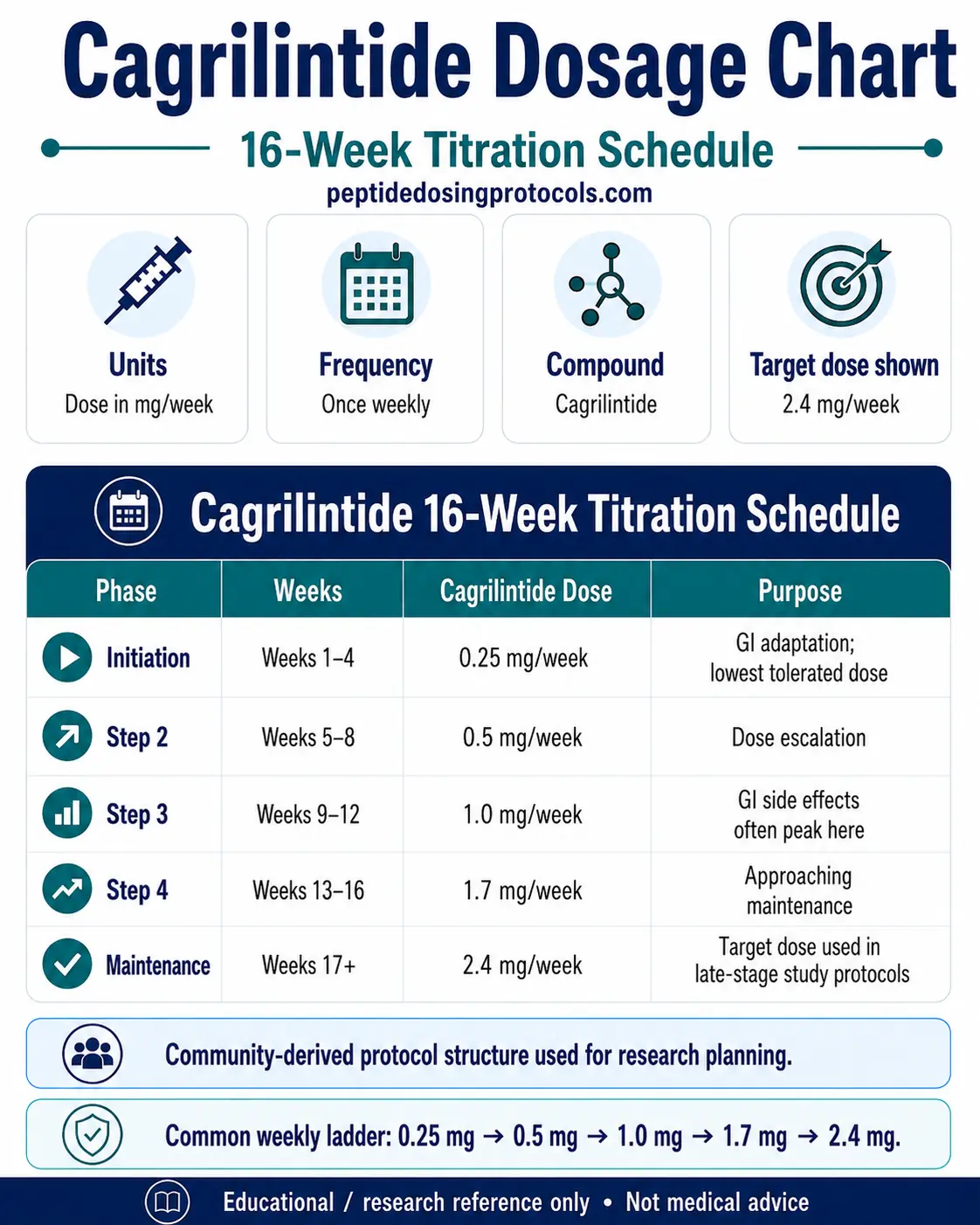
Cagrilintide Dosing & Weekly Titration Schedule (Practical Protocol Logic)
Below is the type of structure you’ll see in a typical cagrilintide titration protocol: weekly step-ups with pauses to let tolerance develop. Even when two people start with the same baseline, they may need different “hold times” at intermediate steps.
Weekly titration: what “good” looks like
In my hands-on protocol reviews, a “good” titration pace typically results in:
- Side effects that are mild and transient (often strongest in the first day or two after a step increase).
- Predictable appetite changes rather than sudden swings.
- Stable meal tolerance (you can consistently eat appropriately sized meals without significant nausea).
How to decide when to hold vs. increase
Most people can only make titration decisions safely using symptom patterning. Use this logic:
- Increase if improving: symptoms are decreasing each week, and you can maintain normal hydration and meal intake.
- Hold longer if symptoms persist: if nausea/reflux/constipation are still clearly active late in the dose cycle, holding can prevent a “stacking” effect.
- Reassess if you’re worsening: if symptoms escalate after a step increase or you can’t eat enough to stay hydrated, the schedule needs to change.
Missed dose logic (what I recommend)
Missed dosing often becomes stressful because people try to “catch up” aggressively. My practical rule is to avoid large rescheduling jumps. Instead:
- Return to the next planned dosing window if you’re close to it.
- Avoid trying to “make up” multiple doses in a short period.
- If you miss long enough to restart, treat it like a fresh start and rebuild tolerance cautiously.
If you want, tell me how many days you missed and your current titration step, and I can help you map a conservative resumption approach.
Cagrilintide vs. Tirzepatide: Why Dose Comparisons Get Confusing
People often search for cagrilintide and tirzepatide dosage together because both are discussed in the context of appetite control and metabolic health. But dosing schedules aren’t interchangeable in a simple “dose-for-dose” way.
Key differences that affect how you should plan
- Mechanism nuance: different target profiles can change how strongly you feel appetite suppression and GI effects at a given step.
- Titration pacing: even when weekly patterns exist, tolerance timelines can differ person to person.
- Side-effect profiles: nausea, reflux, and constipation can appear at different points in the ramp-up.
My rule for avoiding dosing mistakes
When switching products or when you’re trying to infer one schedule from another, don’t translate the numbers directly. Instead, base your plan on:
- your current tolerance (how your stomach responds right now),
- the last step you took without major symptoms, and
- a conservative titration restart if you’re switching.
This is where many people run into problems—especially when they expect the same dose to create the same symptom intensity.
Safety: What to Monitor During Cagrilintide Titration
Safety isn’t only about avoiding “dangerous” events—it’s about preventing preventable issues that derail adherence. In real-world protocol execution, the most common safety-related problems are dehydration from inadequate intake, constipation, and reflux that feeds a cycle of reduced eating.
Daily monitoring checklist
- Hydration: check urine color and frequency.
- GI symptoms: nausea, heartburn, bloating, constipation/diarrhea.
- Meal tolerance: can you finish a reasonable meal without discomfort?
- Weight trend: track weekly averages, not single-day fluctuations.
When to slow down (experience-based triggers)
In my hands-on work, I’ve seen titration pace problems when:
- you keep increasing despite persistent nausea beyond the early window,
- you’re under-eating to “push through,” which worsens constipation and fatigue,
- reflux becomes a daily issue and your meals shrink drastically.
Important constraint: follow a clinician’s guidance
Peptides can affect appetite and GI function significantly. If you have diabetes, kidney issues, history of pancreatitis/gallbladder problems, severe GI disease, or you take glucose-lowering medications, your titration plan should be coordinated with a qualified clinician. This guide is about protocol design logic—not a substitute for medical supervision.
Common Implementation Details That Affect Outcomes
Two dosing plans can have the same titration logic but produce different results due to execution details. I always stress the “boring” variables because they determine consistency.
Consistency beats improvisation
- Use a consistent dosing day if possible (weekly schedule discipline matters).
- Don’t rapidly change injection timing without a reason.
- Plan meals around the first day or two after each step up if that’s when symptoms peak.
Food strategy to reduce side effects
During ramp-up, meal composition often determines whether you feel controlled or miserable:
- Smaller, slower meals typically reduce nausea.
- Lower-fat choices can be easier when gastric emptying feels slower.
- Fiber + hydration helps constipation—but increase fiber gently.
FAQ
What’s the goal of cagrilintide titration?
The goal of cagrilintide titration is to let your body adapt gradually so appetite control improves while side effects remain mild and manageable. Most people do best when dose increases are paced to symptom trends rather than a rigid timetable.
How should I think about cagrilintide and tirzepatide dosage if I’m comparing schedules?
Don’t translate between cagrilintide and tirzepatide dosage as if the numbers are equivalent. Instead, compare tolerance outcomes and use a conservative, tolerance-led titration approach—especially if you’re switching products or restarting after a break.
When should I hold my current step instead of increasing?
Hold longer if GI symptoms are still clearly active late in the dosing cycle, if meal tolerance is deteriorating, or if hydration is hard to maintain. Increasing while symptoms are still ongoing is one of the most common reasons protocols fail.
Conclusion
A strong cagrilintide peptide dosing plan is less about “finding the perfect number” and more about building a titration routine your body can adapt to—week by week—without derailing hydration, meal tolerance, and consistency. And when people search cagrilintide and tirzepatide dosage, the most important takeaway is that schedules aren’t interchangeable; tolerance-led pacing is what keeps things safe and sustainable.
Next step: pick your intended weekly dosing day, write down your starting step and a hold/increase rule based on symptom trends (not guesswork), and track hydration + GI tolerance for the first 2 weeks so you can adjust responsibly before you feel “behind.”
Discussion