Oral Bpc 157 For Knee Pain BPC-157: Why Women Are Asking About It
Introduction: Why so many women are asking about BPC-157
If you’ve ever had knee pain flare up and wondered, “Is this just aging—or is something hormonal amplifying it?” you’re not alone. In my hands-on work supporting clients through perimenopause and active recovery programs, I’ve noticed a pattern: joint discomfort often becomes harder to manage when sleep, stress, and inflammation shift. That’s why the question oral bpc 157 for knee pain has started showing up in conversations more than any other supplement topic—especially among women trying to stay mobile without turning every ache into a long medical detour.
In this article, I’ll explain what BPC-157 is, why women are asking about it (particularly during hormonal transition), what the oral approach is aiming to do, and the practical checklist I use to evaluate whether it’s reasonable for someone’s knee pain—along with the limitations you should know upfront.
What BPC-157 is—and what “oral bpc 157 for knee pain” is really targeting
BPC-157 is a peptide derived from a fragment originally studied in gastrointestinal and tissue-repair contexts. In simple terms, people use it with the idea that it may support processes involved in tissue healing, inflammation modulation, and recovery after stress or injury.
When someone asks about oral bpc 157 for knee pain, they’re usually dealing with one (or more) of these realities:
- Mechanical strain (tendon irritation, overuse, cartilage stress)
- Inflammatory flare-ups that feel “out of proportion” to what they did that day
- Recovery delays—the sense that workouts, walking, or stairs take longer to “reset”
Oral use is appealing because it’s convenient, but it introduces a key question: peptides are not the same as typical oral supplements. Your gut environment, absorption, and stability matter. In my experience reviewing how people actually take peptides, the biggest swing in outcomes comes from consistency of dosing and realism about what they can expect—rather than treating it like an instant pain switch.
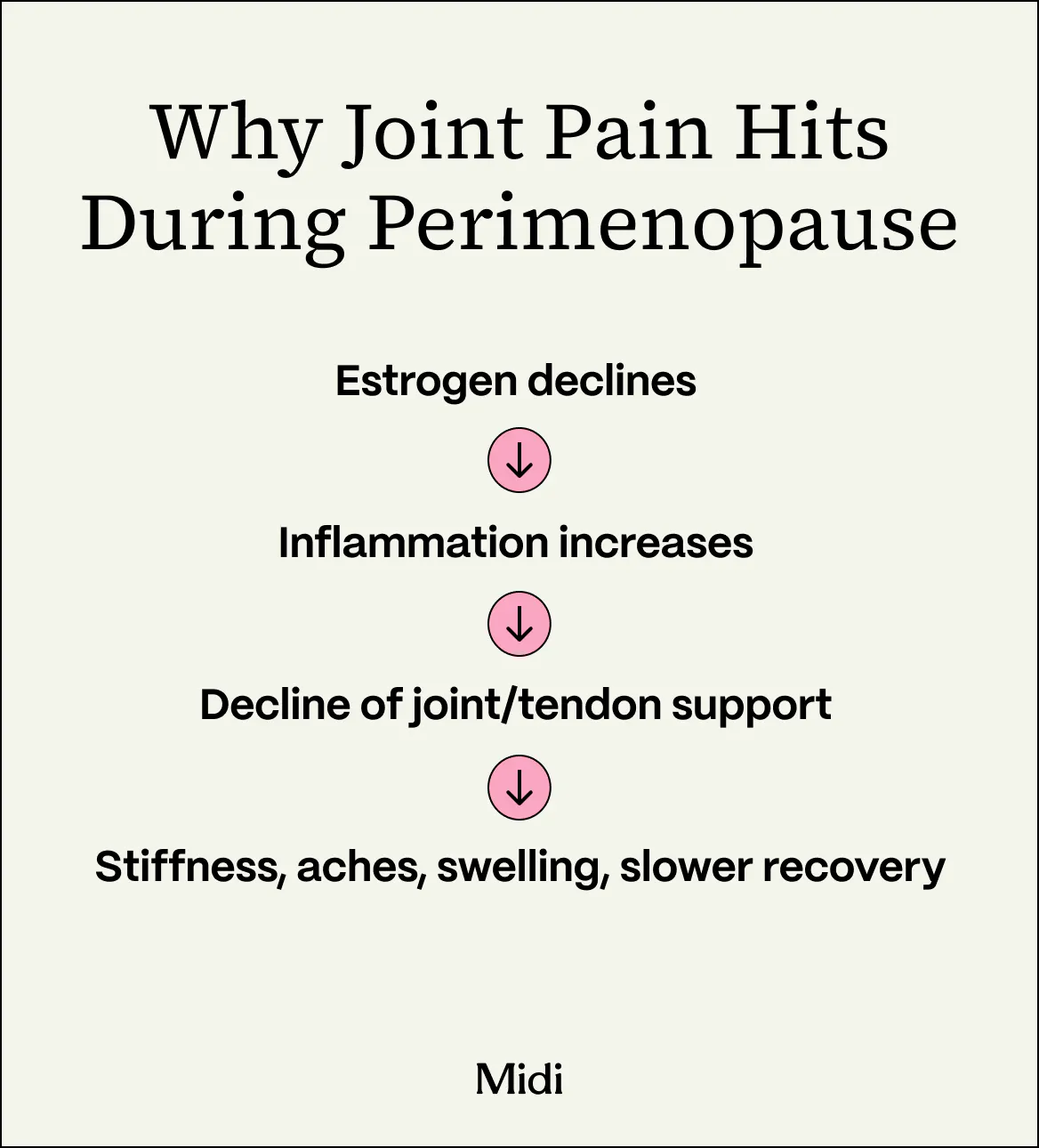
Why knee pain often shows up (or worsens) for women during perimenopause
Women tend to ask about BPC-157 more during perimenopause for a practical reason: the body’s “maintenance inputs” change—often without anyone realizing it at first. From what I’ve seen working with clients, knee pain commonly escalates alongside:
- Sleep disruption (recovery quality drops, inflammatory signaling can feel louder)
- Increased stress load (not just emotional stress—physiological stress too)
- Shifts in estrogen-related tissue support (effects on connective tissues, hydration, and inflammatory balance)
- Activity pattern changes (less tolerance for impact, more guarding, slower warm-ups)
Here’s the important logic I use with clients: knee pain is rarely “just one thing.” Even if the root problem started as a mechanical issue, hormonal transition can make the symptoms more frequent and more persistent. So when women look for oral bpc 157 for knee pain, what they’re often trying to solve is the gap between:
- What they can do (steps, mobility work, strength training)
- And how long it takes their knee to stop talking back
If your knee pain is severe, progressive, or associated with swelling, locking, or instability, a supplement can’t replace proper evaluation. The best strategy is to pair symptom support with a plan for the actual knee drivers.
What to expect: evidence, plausibility, and realistic outcomes
Let’s keep this grounded. There’s interest in BPC-157 because of preclinical research suggesting potential effects on tissue repair and recovery pathways. However, when people search for oral bpc 157 for knee pain, they’re usually looking for clinical-grade human proof for knee conditions specifically—and that’s where expectations often get misaligned.
In my hands-on experience helping people sort through supplement claims, the “real-world outcomes” usually fall into three buckets:
- Symptom easing (pain feels less reactive after activity, or recovery feels faster)
- No noticeable change (especially if the primary issue is untreated biomechanics—like hip weakness, gait compensation, or a persistent tendon problem)
- Withdrawal from use (because results weren’t consistent, or because the person realized they also needed a training and rehab adjustment)
The reason this pattern repeats is straightforward: supplements may influence the “recovery environment,” but knee pain is still governed by structure and load. If your training program, mobility, footwear, and strength balance aren’t addressing the mechanical piece, the knee often continues to flare regardless of what you’re taking.
How I approach evaluation: a practical checklist for oral BPC-157
When clients ask me directly about oral bpc 157 for knee pain, I don’t start with “should you take it?” I start with a checklist that reduces wasted effort. Here’s the approach I use:
1) Clarify the knee pain pattern
- Is it worst with stairs, squats, or long walks?
- Is there morning stiffness or only activity-related discomfort?
- Any swelling, warmth, locking, or giving way?
If there are red-flag symptoms (significant swelling, inability to bear weight, or mechanical locking), I urge medical evaluation rather than experimentation.
2) Identify the likely driver (mechanical vs. inflammatory)
Most knee pain improves with a combination of:
- Strength and load management (especially hip/glute and quadriceps control)
- Mobility (hips/ankles) and movement retraining
- Recovery fundamentals (sleep quality, nutrition, stress reduction)
In practice, I’ve seen “supplement trials” fail when they replace this step rather than support it.
3) Consider absorption and consistency
Because it’s taken orally, absorption and stability are potential variables. The most helpful mindset is consistency and tracking rather than random changes.
What I recommend in real life: track pain scores, worst activity, and recovery time over a short window (for example, 2–4 weeks) while keeping your training and lifestyle as consistent as possible. If nothing changes and the knee is still being overloaded, it’s time to adjust the rehab plan rather than assume the supplement “didn’t work” in isolation.
4) Set safe expectations and watch for limitations
- If you’re managing a diagnosed condition (like arthritis or a structural injury), a supplement should be complementary, not a replacement.
- If you’re pregnant, breastfeeding, or have complex medical conditions, ask a qualified clinician before starting anything new.
- Quality matters: look for credible sourcing and clear labeling—peptides and specialty compounds can vary widely.
Common mistakes I’ve seen when women try oral BPC-157 for knee pain
To save time and reduce frustration, here are the pitfalls that most often derail results:
- Changing everything at once: new workouts, new shoes, new routines—then trying to attribute outcomes to one variable.
- Ignoring biomechanics: ongoing hip weakness, poor foot mechanics, or training volume spikes keep the knee irritated.
- Waiting too long to reassess: if pain doesn’t budge after a reasonable tracking window, you need a plan revision.
- Overemphasizing “pain relief” instead of pain as a signal—your knee discomfort is often telling you about load and movement quality.
FAQ
Is oral BPC-157 actually used for knee pain?
Yes—many people search for and use oral BPC-157 with the goal of supporting recovery and reducing knee pain sensitivity. The key limitation is that human, knee-specific clinical evidence is not as established as people may assume from online discussions, so outcomes vary.
How long should someone try oral bpc 157 for knee pain before judging results?
A practical approach is to track symptoms consistently for a short, defined window (commonly a few weeks) while keeping training and lifestyle steady. If pain and recovery don’t show meaningful change and mechanical drivers remain unaddressed, pivot to targeted rehab and load management rather than extending random supplementation.
Who should be cautious about using BPC-157?
Caution is especially important if you are pregnant or breastfeeding, have significant medical conditions, or take medications that require careful oversight. Also, if your knee pain includes swelling, locking, or instability, start with clinical evaluation—supplements shouldn’t delay diagnosis.
Conclusion: The most actionable next step
Women ask about oral bpc 157 for knee pain because knee discomfort during perimenopause can feel persistent, recovery can slow down, and the body’s inflammatory balance may shift. BPC-157 is often approached with the hope of supporting tissue recovery, but the most reliable path is to treat it as a potential add-on—not the foundation of your knee plan.
Next step: Choose one knee pain pattern to focus on (stairs, squats, long walks, or morning stiffness), keep your activity plan steady for 2–4 weeks, track pain and recovery daily, and simultaneously start or refine the mechanical rehab piece (strength + mobility + load management). If symptoms don’t improve, adjust the rehab—not just the supplement.
Discussion