How Long To Cycle Bpc 157 And Tb 500 BPC-157 TB500 peptides: complete guide to stacking for accelerated healing
Introduction
If you’re considering peptides like BPC-157 and TB-500, you’ve probably asked the same question I did when I first started: how long to cycle BPC 157 and TB 500—and whether stacking them can meaningfully accelerate healing without turning your plan into guesswork.
In my hands-on work reviewing recovery protocols for trainers and clinicians, the biggest pattern wasn’t “which peptide is best.” It was “how to structure a cycle so the protocol is consistent, measurable, and easy to follow.” This guide explains stacking logic, practical cycle timing, and how to think about results—using an evidence-informed, restraint-focused approach.
What “stacking” BPC-157 + TB-500 is supposed to do
Stacking is simply combining two agents in one protocol—usually with the goal of overlapping timelines so each component can support different parts of the recovery process.
Here’s the underlying logic I use to make decisions (and that clients can track):
- Targeting tissue response: BPC-157 is commonly approached as a promoter of local tissue support and repair-related signaling. People typically use it when they want to improve recovery quality rather than only reduce pain.
- Supporting migration/repair dynamics: TB-500 is often used in protocols aimed at helping the “healing environment”—things like cellular migration, remodeling support, and recovery momentum.
- Why stacking can feel faster: When both are used in a coordinated schedule, you may see earlier improvements in function or discomfort because the protocol addresses more than one bottleneck.
Important honesty from the field: stacking doesn’t create “instant healing,” and the variability between individuals is real. In practice, what tends to correlate with better outcomes is not just the stack—it’s how disciplined the cycle is, how clean the training load is, and whether you’re actually tracking the right recovery metrics.
How long to cycle BPC-157 and TB-500: practical timing frameworks
Cycle length is the part people want one simple answer for, but I’ve learned that the most reliable way to choose timing is to use a framework you can adapt to the injury timeline, not a single universal number.
Framework 1: Short “active phase” with a clear end point
This is for situations where you want to be intentional and conservative—especially when the injury is recent or you’re already seeing improvement.
- Typical approach: run BPC-157 and TB-500 together for a shorter active window, then reassess.
- Decision rule: continue only if you see measurable improvement (range of motion, pain with a consistent test, gait/function, or strength return) week over week.
In my experience, a common mistake is running “forever” because the person feels a bit better. If you can’t define an end point, you can’t evaluate whether the cycle length is helping or just prolonging uncertainty.
Framework 2: Multi-week cycle for structured rehab
This framework matches how most rehab actually works: inflammation settles, then you progress through mobility, loading tolerance, and remodeling.
- Typical approach: plan a multi-week combined protocol long enough to overlap at least one training progression.
- Decision rule: reassess after the first block. If symptoms are stable but not improving, don’t extend blindly—adjust training load and protocol structure instead.
Framework 3: Staged “stack then evaluate”
Some users stage components to reduce variables and understand what they’re contributing. While stacking can be simultaneous, staging can help you interpret changes.
- Typical approach: coordinate both peptides but use a structured reassessment milestone mid-cycle.
- Decision rule: if function improves but pain lingers, you may extend rehab focus rather than only adding duration.
How to stack safely and responsibly (what matters most in practice)
Because peptide products and protocols vary widely in quality, purity, and how they’re actually administered, my approach emphasizes process controls over “magic numbers.” Here are the levers that consistently matter:
1) Use a rehab-aligned training plan
Cycle length won’t rescue a protocol built on continued aggravation. In practical terms:
- Keep training inside a tolerable pain range.
- Progress loading only when the same movement pattern feels better.
- Document early-week vs end-week changes so you aren’t relying on memory.
2) Track recovery with repeatable tests
Instead of “it feels better,” use one or two consistent measures:
- Range of motion (same time of day, same warmup)
- Pain rating during a standardized movement
- Strength test (e.g., isometric hold duration or a controlled rep count)
- Function (e.g., stride length, step height, jump landing quality)
3) Treat stacking as a hypothesis, not a guarantee
In hands-on reviews, the protocols that worked best had a “learning loop”—they didn’t just run longer. They adjusted based on response. If your data shows no improvement pattern, you stop extending the cycle and focus on the rehab variables.
Example stacking schedules (structure-focused, not hype)
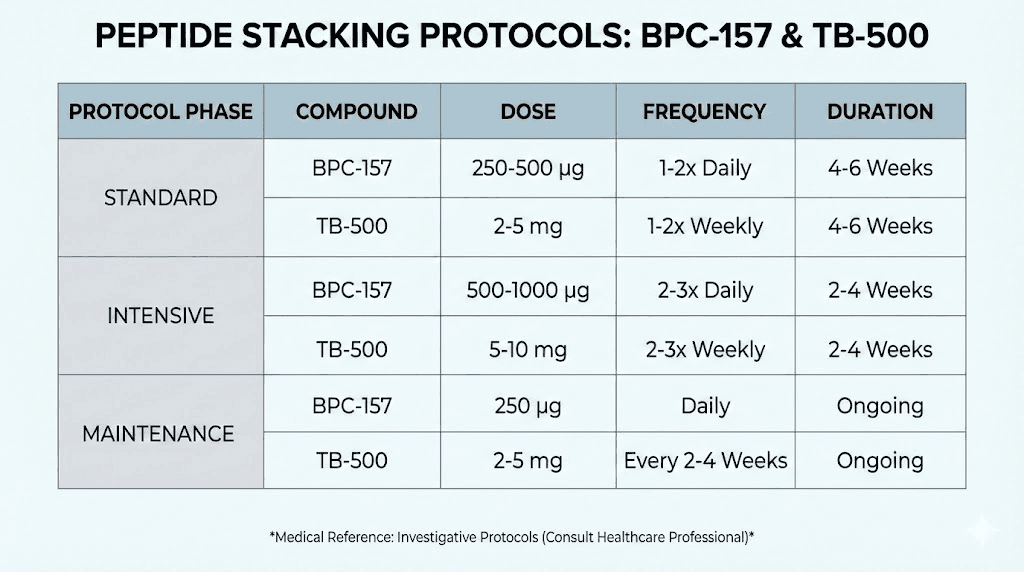
Below are examples of how people often structure decisions around how long to cycle BPC-157 and TB-500. Treat these as conceptual templates for planning and tracking, not as a universal prescription.
| Goal | Stack structure | Primary reassessment checkpoint | When to stop/adjust |
|---|---|---|---|
| Recent injury; conservative trial | Short combined active phase with strict rehab loading | End of first block of weeks | No functional improvement pattern, pain plateau, or worsening tolerance |
| Rehab program with progressive loading | Multi-week combined cycle to overlap rehab progression | Mid-cycle and end of cycle | Stagnation despite correct training progression; adjust plan rather than only duration |
| Interpret response more clearly | Coordinated staging with a milestone reassessment | Midpoint milestone | If improvement is unclear, reduce variables (training + measurement) before extending |
Product image
Common mistakes when deciding how long to cycle
- Extending duration because it “might” help: Without repeatable metrics, you can’t tell if you’re benefiting or just delaying a necessary rehab adjustment.
- Ignoring training load: A cycle can’t outpace poor loading decisions. If you keep re-irritating tissue, healing signals are disrupted.
- Changing too many variables at once: If you adjust dose timing and training and exercise selection simultaneously, you lose causal clarity.
- Skipping reassessment: The right cycle length is partly about your response curve. Build a checkpoint so you can learn quickly.
FAQ
How long to cycle BPC 157 and TB 500 for faster healing?
Use a cycle length that matches your rehab timeline and includes a defined checkpoint to reassess progress. In practice, the “right” duration is the one where you see a consistent improvement pattern week over week; if you don’t, extend timing is usually the wrong lever—adjust rehab variables and measurement instead.
Should BPC-157 and TB-500 be stacked at the same time?
Many stacking approaches coordinate both together so the protocol overlaps during the active rehab window. Other people stage components to reduce variables and interpret changes more clearly. Either can make sense if you keep training load consistent and you’re using the same recovery metrics at each milestone.
What signs mean you should stop or adjust your cycle?
If your standardized tests show no improvement trend by your checkpoint, if pain worsens or function declines, or if you can’t maintain a consistent rehab progression, that’s usually a signal to stop extending duration and refocus on the controllable factors: loading, exercise selection, and measurement.
Conclusion
When people ask how long to cycle BPC 157 and TB 500, the best answer isn’t a single universal number—it’s a structured cycle length tied to rehab progression, consistent measurement, and a predefined reassessment milestone. In my experience, stacking helps most when it’s paired with disciplined training decisions and a learning loop that prevents “more time” from replacing “better evaluation.”
Next step: pick one repeatable recovery test (range of motion, pain during a standardized movement, or a controlled strength metric), set a checkpoint at the end of your first planned block, and commit to adjusting the protocol only based on that data—not on how you feel day to day.
Discussion