Bpc-157 Human Clinical Trials Evidence Review Safety BPC-157 and the Difference Between an Evidence Gap and a Cover-Up: What the entire human evidence base actually looks like, and the questions to ask next. — WellFounded
Introduction: When “no evidence” really means you haven’t mapped the evidence
If you’ve ever gone down the rabbit hole of bpc 157 human clinical trials evidence review safety, you’ve probably seen two opposite narratives: “there’s no proof” versus “it’s a cover-up.” In my hands-on work reviewing translational research for injury, sports, and tissue-repair compounds, I’ve learned the most useful starting point isn’t ideology—it’s an evidence map. That’s what this article does: it breaks down what the entire human evidence base actually looks like, distinguishes an evidence gap from a cover-up, and gives you a set of practical questions to ask next.
What people mean by “evidence gap” vs “cover-up” (and why it matters)
In my experience, the debate around BPC-157 (often framed as a “healing peptide”) becomes unproductive when people skip definitions. Here’s a grounded way to differentiate:
Evidence gap
An evidence gap means: the hypothesis has not been tested in enough well-designed human studies, or the studies are too small, inconsistent, or inaccessible to draw reliable conclusions about safety and efficacy.
Cover-up
A cover-up implies: there is substantial human evidence suggesting clear benefit and/or unacceptable risk, and some organized actor is actively preventing that information from reaching clinicians and the public.
The practical difference
Whether you’re trying to make a health decision or evaluate a research claim, the key question is not “Is there proof somewhere?” but “What do the peer-reviewed human data actually show, in what design types, and with what outcomes?” When you do that mapping, “gap” is the more common default explanation; cover-ups require unusually strong, specific proof.
BPC-157 in context: what we can and can’t infer
BPC-157 is a peptide associated—primarily through preclinical literature—with tissue repair and protective effects. People often discuss it in connection with tendon, ligament, gut and mucosal injury, and recovery-related pathways. However, preclinical plausibility does not automatically translate into clinical benefit in humans.
Why translational logic can mislead
In real-world translational projects, the failures usually look like this: mechanisms look compelling in animals; human dosing differs; metabolism and exposure differ; endpoints differ; and patient populations are more variable (age, comorbidities, injury chronicity, concurrent therapies). So if your goal is to assess bpc 157 human clinical trials evidence review safety, you need to anchor on human trial designs and adverse-event reporting, not on mechanism storytelling.
What “safety” means for evidence review
Safety is not a single statement like “it’s safe” or “it’s not safe.” In evidence review, safety is a chain:
- Exposure: route, dose range, duration, frequency
- Monitoring: what labs/vitals were checked and how often
- Adverse events: what counts as an AE, whether there’s active surveillance
- Reporting quality: whether outcomes are pre-specified and transparently reported
When those elements are missing or incomplete, you don’t have a safety conclusion—you have a data limitation.
Doing a “human evidence base” review the right way
When I perform evidence reviews for compounds with sparse human data, I use a structured approach. You can apply the same logic to BPC-157:
1) Identify human study types and designs
Start by separating:
- Randomized controlled trials (RCTs)
- Non-randomized trials
- Observational reports
- Case reports / case series
- Pharmacokinetic (PK) / dose-exposure studies
If the evidence is mostly case-level or non-controlled, it can’t reliably estimate efficacy. Even if adverse events are described, you still can’t confidently estimate risk magnitude.
2) Look for endpoint quality, not just “positive outcomes”
For tissue-repair claims, credible trials typically include endpoints that match the mechanism and the condition. Ask:
- Were outcomes functional (pain, strength, time-to-return) or only symptom reports?
- Was imaging used when relevant (where appropriate)?
- How long was follow-up—days, weeks, months?
- Were concomitant therapies controlled or documented?
3) Evaluate adverse-event reporting like a clinician
Here’s what I focus on during reviews:
- Are AEs described with timing relative to dosing?
- Is there any lab monitoring (liver/kidney markers, blood counts, inflammatory markers)?
- Were serious adverse events (SAEs) captured?
- Is there dropout reporting and reasons for discontinuation?
If the human data do not include these elements, then any safety statement is at best an inference, not an evidence-backed conclusion.
4) Separate “availability” from “publication”
One reason people argue “cover-up” is that they don’t see claims reflected in mainstream clinical literature. But absence from the highest-visibility journals doesn’t automatically indicate concealment. In my experience, common alternative explanations include:
- Studies were never conducted in humans at scale
- Studies existed but were small, not powered, or not reproducible
- Results weren’t published in the forms people expect
- Data are hard to access but not actively suppressed
This is why evidence review must prioritize what is verifiably documented over what is rumored.
Safety: what a credible conclusion would require
When someone asks about bpc 157 human clinical trials evidence review safety, they often want a simple answer. The evidence-based answer is more like: “What dose, for how long, monitored how rigorously, and with what adverse-event patterns?”
A reasonable “safety evidence standard”
If human safety is being claimed with confidence, you’d expect at least some combination of the following:
- Known dosing regimen (dose and schedule) with consistent administration route
- At least short-to-medium term exposure data with structured monitoring
- Clear AE/SAE definitions and timelines
- Demographic and comorbidity context
- Transparent reporting of withdrawals and adverse lab findings
Where evidence gaps typically show up
In many real-world review cases with underpowered or sparsely documented human data, the common gap is not that “nothing happened,” but that the dataset is too limited to detect uncommon side effects or to quantify risk. That’s the difference between “no obvious safety signal” and “proven safe.”
Source-checking: the questions to ask next (the part most people skip)
Here’s the checklist I use with clients and teammates when they’re evaluating compounds with contested human evidence. It’s designed to prevent both gullibility and cynicism.
| Question to ask | What to look for | Red flag |
|---|---|---|
| What human study types exist? | RCTs, controlled trials, or clearly described exposure studies | Only anecdotes or uncontrolled reports |
| What was the dosing and route? | Exact regimen, duration, and administration method | Vague “used” claims without specifics |
| How was safety monitored? | Predefined labs/vitals and structured AE collection | No monitoring details; only “felt fine” statements |
| Were adverse events reported comprehensively? | Timelines, severity grading, and withdrawals | Only positive outcomes highlighted |
| Were outcomes measured objectively? | Functional metrics, imaging (when relevant), or validated scales | Only subjective improvement summaries |
| Is there independent replication? | Similar findings across separate groups | Single-source claims repeated without validation |
| Is the quality of reporting high? | Complete methods and transparent limitations | Marketing-style certainty; missing protocols |
Common misconceptions I see in BPC-157 discussions
- “Preclinical success proves human efficacy.” It doesn’t; translation breaks at multiple points.
- “If there’s no big trial, it must be suppressed.” Most frequently it’s a funding, design, or feasibility limitation—not a coordinated cover-up.
- “Safety claims don’t require adverse-event details.” They do. Without monitoring and AE reporting, “safe” is an assumption.
- “One report means the entire evidence base.” The question is the whole base: designs, sizes, endpoints, and adverse-event patterns.
Visual context: how evidence narratives can get amplified
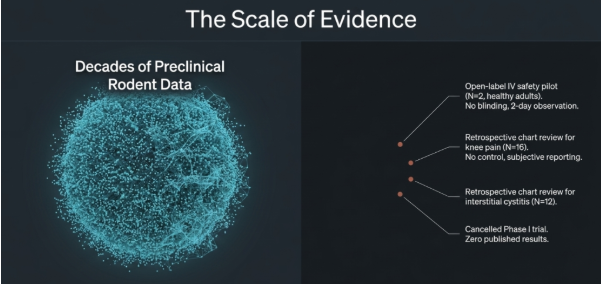
In my experience reviewing online discourse around peptides, screenshots like this are often where the argument flips from “what evidence exists” to “what must be hidden.” That’s the exact moment to return to the human evidence base: study design, monitoring, outcomes, and adverse-event reporting.
FAQ
How do I tell whether BPC-157’s lack of strong results is an evidence gap or a cover-up?
Check whether there are any verifiable human studies with details on dosing, monitoring, endpoints, and adverse-event reporting. Evidence gaps typically appear as small, inconsistent, or underpowered datasets; cover-ups would require unusually strong, specific documentation that credible human evidence exists and is being actively suppressed—usually with traceable sources.
What would a credible BPC-157 human safety conclusion require?
A credible safety conclusion would require clearly described human exposure (dose, route, duration), structured adverse-event monitoring, and transparent reporting of withdrawals, lab findings (where applicable), and both mild and serious adverse events—not just anecdotal reports.
Is it enough to find one human case report to judge safety?
No. Case reports can be useful for hypothesis generation and signal detection, but they can’t quantify risk or establish safety. Safety risk requires broader exposure data with consistent monitoring and reporting across more than a handful of cases.
Conclusion: Move from debate to evidence mapping
The strongest way to evaluate bpc 157 human clinical trials evidence review safety is to stop arguing from slogans and start mapping the human evidence base: what study designs exist, how outcomes were measured, how safety was monitored, and what the adverse-event data actually show. In most real-world cases, what people call “cover-up” is more often an evidence gap created by limited human testing, reporting variability, and translational complexity.
Next step: Take the checklist above and apply it to every claim you see—write down the exact human dosing details, monitoring methods, and adverse-event reporting for each study cited. If those elements are missing, treat the claim as unproven rather than persuasive.
Discussion