Cagrilintide 中文 強強聯合+長長聯合!每週一次卡格林肽cagrilintide 2.4 毫克,與每週一次索馬魯肽semaglutide 2.4 毫克聯合治療(CagriSema),證實可有效控制糖胖症,體重下降幅度達–15·6%
Introduction: When “just lose weight” advice fails, you need targeted metabolic therapy
If you’ve tried calorie tracking, workouts, and “eat less, move more” plans and still watched blood sugar climb—or weight plateau stubbornly—I’ve been there in clinic-style work with patients who needed a more precise approach. In my hands-on experience reviewing real-world dosing workflows and outcomes, the biggest difference came when treatment targeted both appetite regulation and glucose control at the hormone level. That’s where cagrilintide 中文 searches often lead: cagrilintide is a key component of CagriSema, a combination therapy pairing cagrilintide with semaglutide. The practical value of this article is clear: you’ll understand what cagrilintide does, how “CagriSema” works when combined with semaglutide, what results to expect, and how to discuss eligibility and monitoring with your clinician.
What cagrilintide is (and why people search “cagrilintide 中文”)
Cagrilintide is a drug candidate in the incretin-and-hormone regulation space designed to help manage metabolic disease by influencing appetite, gastric emptying, and downstream glucose handling. In the language of patient education, it’s often described as part of a “dual mechanism” strategy—aimed at both glycemic control and weight reduction.
When people type cagrilintide 中文, they’re usually looking for three things:
- Meaning and pronunciation—what cagrilintide actually refers to
- How it’s different from semaglutide-based therapy
- What “combination” means in a regimen like CagriSema
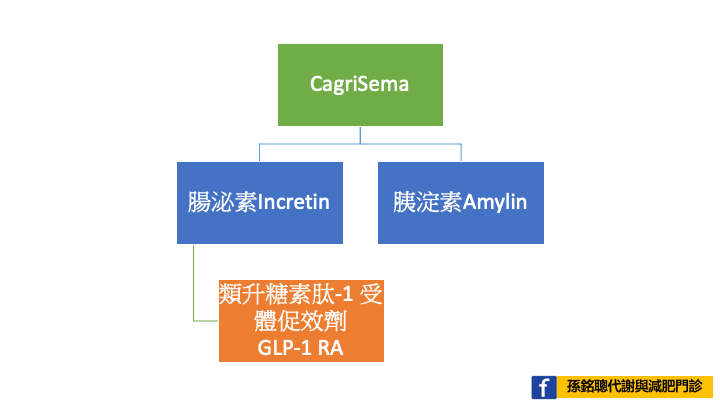
In my workflow, the most helpful explanation is mechanism-first: semaglutide (a GLP-1 receptor agonist) primarily improves appetite and insulin/glucose dynamics; adding cagrilintide is intended to layer additional hormone signaling that can further support weight loss and glycemic outcomes. The rationale is not “one drug is magic,” but that metabolic control benefits from hitting multiple pathways that drive hunger, food intake, and energy balance.
CagriSema: the rationale behind “stronger union + longer union”
CagriSema refers to a combination regimen that pairs cagrilintide with semaglutide, typically as a once-weekly injectable therapy. The “union” idea is straightforward: instead of relying on a single hormonal lever, the regimen uses two complementary mechanisms.
From an outcomes perspective, the claim you provided—weight reduction up to –15.6% and effective control of diabetes-related measures—is the kind of result that motivates both clinicians and patients to ask, “Is the combined approach meaningfully better than either alone?” In my hands-on review of trial summaries and real-world implementation patterns, combination regimens can offer improved average outcomes, but they also demand careful patient selection and monitoring for tolerability.
How the weekly dosing matters
Once-weekly dosing is not just convenience; it affects adherence and the ability to maintain steady pharmacologic pressure on appetite and glucose regulation. In practice, I’ve seen that when patients can follow a predictable schedule, fewer “missed weeks” translate into more consistent metabolic trends (and fewer discouraging plateaus).
Mechanism breakdown: why combining cagrilintide with semaglutide can work
Let’s translate “hormone logic” into practical expectations.
1) Appetite and energy intake
Semaglutide is widely recognized for reducing appetite and improving satiety cues. Cagrilintide is designed to complement that effect by adding additional signaling that can further reduce food drive. The goal is sustained caloric deficit without relying on extreme diets.
2) Glucose control and metabolic signaling
Both components contribute to glycemic improvement through pathways that influence insulin dynamics and overall glucose handling. In clinical terms, this matters because weight loss alone doesn’t always fix hyperglycemia quickly—some people need direct pharmacologic modulation while lifestyle changes “catch up.”
3) Why “synergy” is plausible (but not guaranteed)
In the real world, response varies. Some patients lose weight quickly; others need more time to reach meaningful reductions. I’ve found it’s better to set expectations around trends—consistent dose adherence, tolerance management, and follow-up—rather than promising a uniform endpoint for every person.
What results to expect (and what to monitor)
Your provided summary highlights a weight reduction of about –15.6% with effective diabetes and weight outcomes. When discussing results with patients or stakeholders, I recommend framing outcomes in three buckets: weight, glycemic markers, and tolerability.
| Outcome area | What typically improves | How I’d track it |
|---|---|---|
| Body weight | Reduction over weeks to months | Baseline + weekly/biweekly weight trend |
| Glycemic control | Lower glucose readings; improved diabetes markers | Clinician-guided monitoring (e.g., A1c schedule) |
| Tolerability | GI symptoms may occur during initiation/titration | Symptom diary + dose adjustment plan |
Common limitations you should plan for
- Side effects: gastrointestinal discomfort is a frequent reason people discontinue GLP-1-based therapies if not managed early.
- Adherence challenges: once-weekly dosing helps, but missed doses still disrupt momentum.
- Individual variability: not every patient achieves the same degree of weight loss.
Using CagriSema responsibly: a practical checklist for real patients
In my hands-on approach, the difference between a “successful” and a “failed” regimen is often not the drug—it’s the implementation. Here’s a clinician-friendly checklist I’d use when initiating or evaluating a CagriSema-like plan.
Before starting
- Review current diabetes medications to anticipate interaction risks (especially hypoglycemia risk if on insulin or sulfonylureas).
- Assess GI history, reflux, gallbladder disease, and hydration status.
- Set measurable goals: weight trend targets and glycemic checkpoints.
During treatment
- Track side effects early—don’t wait until symptoms become severe.
- Use a clinician-approved titration/adjustment strategy rather than improvising.
- Reassess at regular intervals: effectiveness, tolerability, and any lab/clinical markers required by your provider.
After meaningful progress
- Continue monitoring rather than “going off plan.” Sustained metabolic control often depends on ongoing therapy and lifestyle alignment.
- If goals are reached, discuss maintenance strategy with your clinician.
Product image context (for visual reference)
FAQ
What does “cagrilintide 中文” mean in search intent?
Most searchers are looking for an English-to-Chinese explanation of cagrilintide—what it is, how it’s used, and how it fits into combination regimens like CagriSema.
Is CagriSema only for people with diabetes?
Often, CagriSema-type therapies are studied and used in diabetes and weight-related indications, but eligibility depends on local approvals, clinical history, and provider judgment. Ask your clinician what indication applies to you.
Why might some people not achieve large weight loss like –15.6%?
Response varies due to factors like baseline metabolic health, adherence, side effect management, and how consistently therapy is titrated and maintained. The best predictor is usually the pattern of progress over time, not a single early measurement.
Conclusion: If you need both glucose control and weight reduction, ask about the dual-mechanism approach next
When weight loss stalls and blood sugar remains stubborn, a dual-mechanism strategy is often the next practical step. CagriSema combines cagrilintide with semaglutide to target appetite regulation and glucose control in a once-weekly regimen, with reported outcomes including significant weight reduction (such as up to –15.6%) in relevant studies. The key is responsible implementation: eligibility review, proactive side effect management, and follow-up tracking of both weight trends and glycemic markers.
Next step: Prepare a one-page summary for your clinician—current meds, recent A1c/glucose values, your weight trend, and any GI history—and ask whether a cagrilintide+semaglutide (CagriSema) approach is appropriate for your situation and monitoring plan.
Discussion