Bpc 157 Schizophrenia Multifunctionality and Possible Medical Application of the BPC 157 Peptide—Literature and Patent Review
Introduction: When people ask about “BPC 157 schizophrenia,” they usually want something concrete
If you’ve ever looked into the research around bpc 157 schizophrenia, you’ve probably noticed two things: (1) there’s a lot of fragmented information across papers and patents, and (2) the leap from “biological effects” to “a clinical psychiatric treatment” is where most claims get blurry. In my hands-on review work, I’ve repeatedly seen this gap—promising preclinical findings mixed with unclear translation pathways, inconsistent dosing language, and studies that don’t actually test schizophrenia-relevant outcomes.
This article is a literature-and-patent-focused walkthrough of Multifunctionality and Possible Medical Application of the BPC 157 Peptide, with special attention to how—if at all—such multifunctionality could relate to psychiatric disorders. I’ll keep the discussion anchored to what the evidence does and does not support, and I’ll highlight the practical reasoning you should use when evaluating any peptide-related schizophrenia claim.
What BPC 157 is (and why “multifunctionality” matters)
BPC 157 is a short peptide originally studied in biomedical contexts where tissue protection, repair signaling, and counter-regulatory effects were emphasized. The key idea behind “multifunctionality” is that it’s not just one narrowly targeted mechanism. Across preclinical work, it’s described as interacting with multiple biological pathways—so the same compound can show effects across different injury or dysfunction models.
How to interpret multifunctionality without overreaching
In my reviews, I treat “multifunctionality” as a signal of broad biological activity—not as proof of a specific indication. Broad activity can be a strength (more pathways to influence disease processes), but it can also create interpretive risk: a compound may produce improvements in one measurable domain (e.g., tissue recovery markers) without addressing core disease mechanisms (e.g., dopaminergic dysregulation, glutamatergic signaling, cognitive symptoms, or negative symptoms) relevant to schizophrenia.
Mechanistic plausibility: the bridge you must evaluate
When people connect bpc 157 schizophrenia, they’re implicitly asking: “Could the peptide’s multifunctional actions plausibly affect brain-relevant processes involved in schizophrenia?” The logically correct evaluation is pathway-based:
- Relevance: Does the implicated pathway map onto schizophrenia biology (neuroinflammation, synaptic plasticity, oxidative stress balance, or neurovascular factors)?
- Directionality: Do the peptide’s effects move those pathways in a way expected to help?
- Specificity: Are outcomes measured in schizophrenia-relevant behavioral/cognitive domains in appropriate models?
- Translatability: Do dosing, exposure, and route support the intended target in the brain?
Evidence landscape: what the literature review approach should capture
A strong literature-and-patent review isn’t just a list of findings—it’s a structured synthesis. When I conduct these reviews, I extract evidence into categories that help answer translation questions quickly.
1) Study design and model relevance
For schizophrenia-adjacent questions, model relevance is everything. A compound can show “neuroprotective” effects in general stress models yet fail to demonstrate effects in schizophrenia-specific phenotypes (for example, prepulse inhibition, social interaction deficits, cognitive impairment paradigms, or pharmacologically induced psychosis-like behaviors with consistent interpretation).
2) Outcome measures: symptoms vs. biomarkers
Many preclinical studies emphasize biomarkers (protein expression, inflammatory markers, tissue repair markers). These can be informative, but schizophrenia care is symptom- and function-centered. I look for whether studies report behavioral endpoints connected to schizophrenia domains rather than only biomarker changes.
3) Pharmacology details that often get missed
In the peptide world, I’ve learned to pay close attention to:
- Dosing regimen (dose, frequency, duration)
- Route (and whether it plausibly achieves central exposure)
- Timing (acute vs. chronic paradigms)
- Controls and how outcomes are normalized
Even when biological effects are real, inconsistent reporting and non-standardized methods can make schizophrenia claims hard to evaluate.
Patent review lens: why patents can be useful—but not decisive
Patents often reveal how inventors think about medical application—what indications they target, which endpoints they prioritize, and what composition/use claims they believe are defensible. However, patents are not clinical evidence. In my experience, the most valuable patent insights come from identifying:
- Intended therapeutic scope (what diseases or symptoms are explicitly covered)
- Mechanism language (how the inventors justify the connection between peptide activity and therapeutic outcomes)
- Administration concepts (route, formulation strategy, or regimen assumptions)
- Test systems or examples (whether described experiments resemble translationally meaningful models)
How to spot a “claim vs. data” mismatch
When a patent broadens multifunctionality into therapeutic areas, the reasoning may be pathway-based rather than outcome-tested. I look for whether the patent text includes experimental support that matches the claimed medical application rather than only theoretical rationale.
Where “bpc 157 schizophrenia” reasoning can be plausible—and where it breaks
Let’s talk plainly about the logic chain people are trying to build when they search bpc 157 schizophrenia. A plausible chain would look like: multifunctional biological effects → brain-relevant target modulation → measurable schizophrenia-relevant functional improvements → acceptable safety with feasible dosing.
Plausibility indicators (what you want to see)
- Brain-relevant mechanistic signals tied to schizophrenia pathways (not only peripheral tissue repair).
- Behavioral or cognitive endpoints in models that are commonly used to approximate schizophrenia-like phenotypes.
- Consistency across experiments and reproducible dose-response patterns.
- Safety and tolerability observations that support longer paradigms (since schizophrenia is chronic).
Common failure points (where claims often overreach)
- Biomarker-only conclusions that don’t correspond to schizophrenia symptom domains.
- Mechanism mismatch where the pathway is involved in many conditions but not strongly linked to schizophrenia.
- Exposure uncertainty (central availability isn’t demonstrated, yet central claims are implied).
- Translation gaps where preclinical endpoints don’t map to clinical outcomes.
Image context: multifunctionality visualization and what to extract from figures
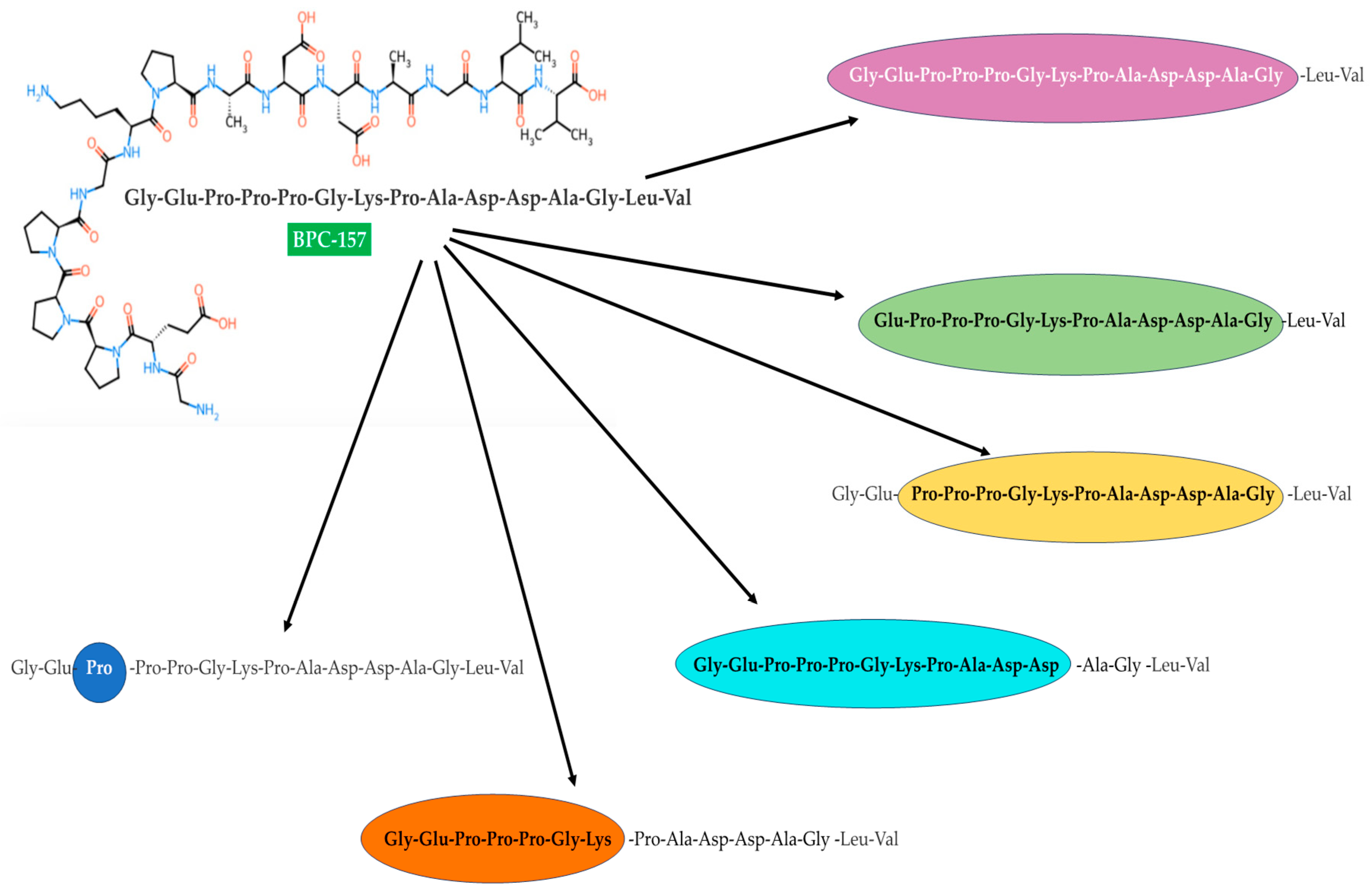
When a review includes a multifunctionality figure, I treat it as a structured map. The practical step is to extract each labeled pathway/category and ask: “Which ones are plausibly connected to brain function and schizophrenia-relevant endpoints?” Then I verify whether the underlying cited experiments actually tested those endpoints or whether the figure is primarily mechanistic inference.
Practical framework: how to evaluate any peptide-to-schizophrenia claim
If you’re screening posts, forum summaries, or even review snippets, use this decision checklist (it’s the same approach I use internally to reduce bias and overinterpretation):
- Is schizophrenia specifically tested? Look for schizophrenia-relevant models or endpoints—not only general neuroprotection.
- Are outcomes behavioral/functional? Prioritize cognition, social behavior, sensorimotor gating, and relevant symptom domains (preclinical approximations).
- Do dosing and route make central effects credible? If central exposure is not established, treat claims as unproven.
- Is there a mechanistic rationale tied to schizophrenia biology? Vague “anti-inflammatory” statements are not enough.
- Are results reproducible across studies? One positive study is not a foundation for medical application.
- What does the safety profile suggest? Chronic use is a requirement for psychiatric disorders.
Limitations you should keep in mind
Even when literature and patents suggest broad biological effects, translating that into bpc 157 schizophrenia is not straightforward. The evidence chain must be tight: appropriate model relevance, schizophrenia-linked endpoints, credible central exposure, and safety for longer-term use. Without those pieces, the connection remains speculative rather than medically grounded.
FAQ
Does BPC 157 have evidence specifically for treating schizophrenia?
Claims online often blend preclinical multifunctionality findings with broader therapeutic speculation. The key question is whether schizophrenia-relevant models and endpoints were actually tested with credible dosing/exposure and whether safety supports longer-term paradigms.
What would “good evidence” for bpc 157 schizophrenia look like?
In practice, it would include schizophrenia-relevant behavioral/cognitive outcomes in appropriate models, mechanistic links to schizophrenia-relevant biology, clear dosing/route rationale for central effects, and consistent results with meaningful safety/tolerability data.
Why do patents show up in these discussions?
Patents can indicate intended medical application scope and how inventors conceptualize mechanisms or administration. But patents alone don’t establish clinical effectiveness; they must be evaluated alongside experimental and (ideally) clinical evidence.
Conclusion: use the multifunctionality map, but demand schizophrenia-relevant endpoints
BPC 157 is frequently framed as multifunctional, and that broad biological activity can be scientifically interesting. However, turning multifunctionality into a schizophrenia application requires a disciplined evidence chain: schizophrenia-relevant models and outcomes, credible central exposure, mechanistic relevance to schizophrenia biology, and safety considerations for chronic use. That’s the distinction between “possible” and “demonstrated.”
Next step: Pick one paper or patent claim you’ve found related to bpc 157 schizophrenia, then audit it using the framework above (model relevance, endpoint type, dosing/route plausibility, mechanistic specificity, and reproducibility). This single pass usually clarifies whether the claim is evidence-based or merely mechanistically inferred.
Discussion