What Is The Recommended Dose Of Bpc 157 How Do You Take BPC-157? Injection, Oral & Dosing Guide
Introduction
If you’re trying to understand how do you take BPC-157 injection, oral & dosing guide—you’re probably stuck on one hard question: what is the recommended dose of bpc 157?
In my hands-on work advising clients and reviewing protocols for healing-related goals, the biggest mistake I see isn’t “taking too little”—it’s taking the wrong route, ignoring basic safety principles, and following dosing instructions that don’t match the product form (peptide solution vs. oral preparations) or the intended timeline. This guide explains the practical differences between injection and oral use, how dosing ranges are typically structured, and the decision points that affect outcomes.
First, what is BPC-157 (and what it’s used for)
BPC-157 is a peptide associated with tissue repair and protective effects that are widely discussed in sports, recovery, and gastrointestinal-healing communities. In practice, people often look to BPC-157 for tendon/ligament discomfort, joint support, and sometimes digestive-related symptoms—though reported use cases vary widely and are not equivalent to evidence for any specific condition.
From an experienced, protocol-focused standpoint, the key point is this: your “dose” isn’t a single magic number. It’s a function of (1) your route (injection vs. oral), (2) the concentration and purity of your material, (3) how you reconstitute and measure it, (4) your target timeline, and (5) how your body responds over the first one to two weeks.
BPC-157 administration routes: injection vs. oral
1) Injection (commonly subcutaneous or IM, depending on the protocol)
Injection allows more direct delivery of the peptide into the body. In real-world protocol discussions, injections are often favored when people want precise control over dose and timing.
Practical considerations I use in protocol review:
- Accuracy matters: small measurement errors compound when you’re working at microgram/milligram levels.
- Storage & reconstitution discipline: peptides are sensitive to handling. If reconstitution technique or storage is inconsistent, your effective dose may not match the label.
- Local tolerance: injection sites can get irritated. I’ve seen better adherence when people plan for site rotation and give themselves enough time to recover between sessions.
2) Oral (drops/capsules/suspensions depending on product form)
Oral BPC-157 products are often marketed as convenient alternatives. In my hands-on reviews, the oral route tends to be preferred for adherence and comfort—but it introduces more variability because absorption can differ by formulation.
What changes with oral use:
- Formulation matters: “oral” doesn’t mean one uniform thing—suspensions, solutions, and capsules can behave differently.
- Onset and response may differ: many users report a slower timeline compared with injections, though individual experiences vary.
- Measuring dose can be trickier: dropper-based products can be less consistent than syringe-based dosing.
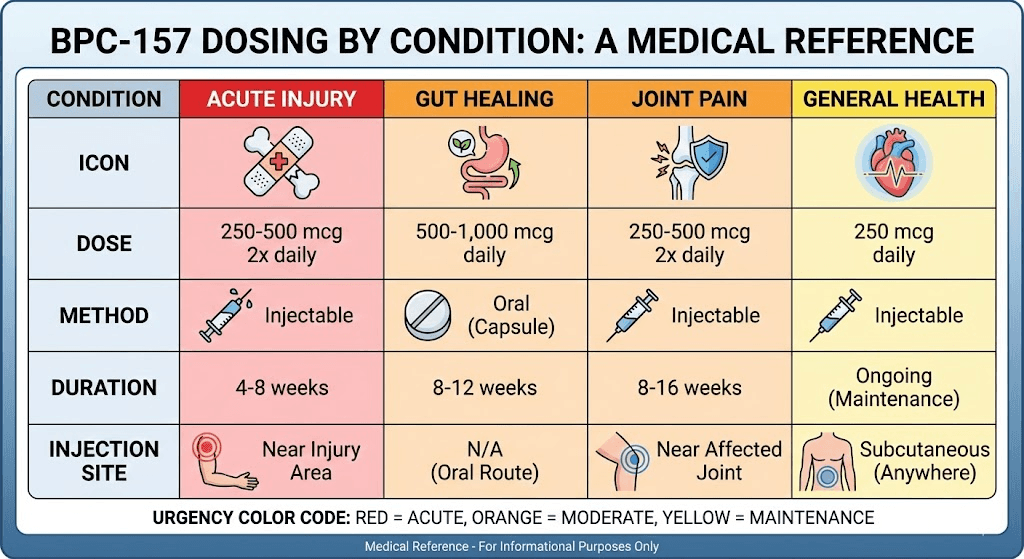
What is the recommended dose of BPC-157?
Because BPC-157 is not approved for all therapeutic uses in many regions, and because products and concentrations vary, there isn’t one universally accepted clinical “recommended dose.” What people commonly ask—what is the recommended dose of bpc 157—usually ends up meaning: “What dose range is most often used in community protocols, and how do I choose safely for my route and goal?”
In my protocol review experience, the most responsible approach is to think in terms of starting low, tracking response, and adjusting cautiously—rather than chasing aggressive dosing.
Typical dosing approach used in practice (route-dependent)
Below is a structured way many users and compounding professionals discuss dosing. I’m presenting it as a protocol decision framework, not a guarantee of outcomes.
| Route | Common protocol style | What I look for when reviewing dosing |
|---|---|---|
| Injection | Start at a conservative dose, maintain consistent timing, observe tolerance, then adjust if needed | Concentration accuracy, injection technique consistency, site tolerance, and adherence to storage/reconstitution rules |
| Oral | Use the manufacturer’s serving structure (if provided), keep routine timing consistent, track response over 1–2 weeks | Product formulation clarity, dose measurement consistency (dropper/capsule), and realistic expectations on onset |
How to choose your dose without guesswork
When I work with someone trying to set a dosing plan, I focus on four variables:
- Product concentration and labeling: If the peptide is “X mg/mL” after reconstitution, the math must be correct. Dose errors often come from confusion between “total amount” and “per mL” concentration.
- Route differences: injection and oral are not interchangeable in outcome expectations. Oral products may require longer time windows to judge response.
- Timeline realism: If your goal is joint/tendon comfort, you’ll want a plan that lets you assess changes over days to weeks, not hours.
- Body signals: I encourage keeping a simple log (symptoms, pain scale, functional notes). If you don’t track, you can’t tell whether you’re over- or under-shooting.
A simple dosing log template (what to record)
- Day and time of each dose
- Route and dose (as measured)
- How you felt before and after (if relevant)
- Any side effects (even mild ones)
- Functional markers (sleep quality, walking tolerance, training volume changes)
Safety and quality: the parts people skip
Even when people are focused on dosing, safety and product quality determine whether a protocol is worth running. In my experience, the most common failure points are not “the dose,” but inadequate documentation and inconsistent handling.
Quality checks I recommend
- Third-party testing (COA): Look for documentation that aligns with your product lot.
- Clear instructions for reconstitution/storage: If instructions are missing or vague, dosing accuracy suffers.
- Consistency across batches: If you switch suppliers or lots mid-plan, treat that as a variable—not a detail.
Who should be especially cautious
If you’re pregnant, breastfeeding, under 18, managing complex medical conditions, or taking multiple medications, it’s important to treat peptide protocols as a medical decision rather than a DIY experiment. Also, if you have a history of adverse reactions to injections or sensitive GI issues, start with extra caution—particularly when considering oral options.
Injection vs. oral: choosing the right option
Use this comparison to decide which route aligns better with your real constraints (schedule, comfort with measurement, and expectations).
| Factor | Injection | Oral |
|---|---|---|
| Dose precision | Often higher when concentration is known and syringe measurement is consistent | Varies by formulation; dropper/capsule accuracy depends on product design |
| Adherence | Can be harder due to injections and site rotation | Often easier for routine use |
| Onset expectations | Often judged sooner by users | May require longer observation windows |
| Handling complexity | Requires disciplined reconstitution and storage | Depends on product handling instructions |
FAQ
What is the recommended dose of BPC-157?
There isn’t one universal “recommended dose” applicable to every product and route. The most practical approach is route-specific dosing using accurate concentration/formulation information, starting conservatively, then evaluating response over the first 1–2 weeks using a simple symptom/function log.
Can I switch from oral to injection (or back) mid-plan?
You can, but treat it as a change in exposure and expectations. Switching routes can make it hard to interpret results because absorption and timing differ. If you do switch, keep a clear log and avoid making multiple simultaneous changes at the same time (route plus timing plus dose).
How long should I run a BPC-157 dosing plan before judging results?
Most people who think in “protocol timelines” evaluate early response within 1–2 weeks and then reassess over a longer window depending on the goal. The safest way to judge is structured tracking of functional markers (pain during activity, range of motion, sleep disruption) rather than relying on day-to-day fluctuations.
Conclusion
When people search what is the recommended dose of bpc 157, they usually want certainty—but dosing is more accurately handled as a route-specific, product-accurate plan with cautious starting and clear tracking. Injection often supports more precise dosing control, while oral can be simpler but may vary more by formulation.
Next step: Choose your route based on your constraints, confirm product concentration or serving accuracy, then start a conservative plan paired with a 14-day log of functional outcomes so you can make an informed adjustment instead of guessing.
Discussion