Recommended Dose Of Bpc 157 And Tb 500 BPC-157 TB500 peptides: complete guide to stacking for accelerated healing
Introduction: Why “stacking” peptides feels promising—and also risky
If you’ve ever dealt with a slow-to-heal tendon, a stubborn muscle strain, or post-procedure recovery that seems to stall for weeks, you’ve probably looked into peptide stacks like BPC-157 TB-500. The appeal is clear: people search for a “stacking” approach hoping to accelerate healing. But the real question I see come up every time—especially from trainees and active professionals—is the same: what’s a recommended dose of bpc 157 and tb 500 that’s sensible, and how do you stack them without making recovery worse?
In this complete guide, I’ll walk you through how BPC-157 and TB-500 are commonly discussed in the performance and wellness community, how stacking is typically structured, what dosing ranges people often reference, and the practical cautions I apply in real-world planning. You’ll leave with a clear framework for thinking about dosage, timing, and monitoring—without the hype.
What BPC-157 and TB-500 are (and what “stacking” is trying to do)
BPC-157 is commonly described as a peptide associated with tissue repair and recovery support. In practical discussions, people use it with the goal of improving processes involved in damaged tissue—especially when the injury feels “stuck” after the initial inflammatory window.
TB-500 (often discussed as “thymosin beta-4” related) is frequently framed as a support peptide for repair pathways, recovery environment, and mobility-related outcomes. When people talk about “stacking,” they’re usually trying to combine what they believe are complementary effects: one aimed more directly at local tissue repair processes, and the other aimed more at recovery environment and regeneration support.
Why stacking is popular
- Synergy theory: People assume two peptides may influence overlapping but not identical repair pathways.
- Structured protocol: A stack gives users a plan: daily dosing, a defined duration, and a “next step” phase.
- Outcome-driven experimentation: Many users start with one peptide, then add the other to see if recovery speed improves.
What stacking does not guarantee
In my experience planning recovery protocols for active people, the biggest misconception is assuming a stack overrides biology. Healing is affected by blood supply, mechanical load management, sleep, nutrition, and the exact injury type. Peptides (or any supplement strategy) are tools, not switches.
How to think about a recommended dose of BPC-157 and TB-500 (practical dosing framework)
Because these peptides are not approved for this kind of off-label use in many places, you’ll often see widely varying dosing schedules online. Instead of pretending there is one universally “correct” answer, I’ll give you a practical dosing framework that matches how people actually build protocols, plus the guardrails I use to reduce avoidable mistakes.
Key point: When you see the phrase “recommended dose of bpc 157 and tb 500,” understand it as “commonly used reference ranges within the bodybuilding/wellness community,” not as medically prescribed dosing.
Common community dosing patterns (not medical advice)
Across forums and user reports, the most typical approach is:
- BPC-157: more frequent dosing (often daily), because users treat it like a “recovery support” peptide throughout the active phase.
- TB-500: less frequent dosing (often multiple days apart), because users treat it like a longer-acting support peptide.
When people discuss “stacking,” they commonly structure the protocol into an active phase (where both peptides are used) and sometimes a follow-up phase (where one is continued or the frequency is changed). The rationale is usually to align dosing with how users perceive the acute-to-subacute transition in healing.
A reasonable “starting protocol” template
Below is a template many people use as a baseline before adjusting based on tolerance and progress. I’m presenting it as a conceptual planning structure, not a prescription.
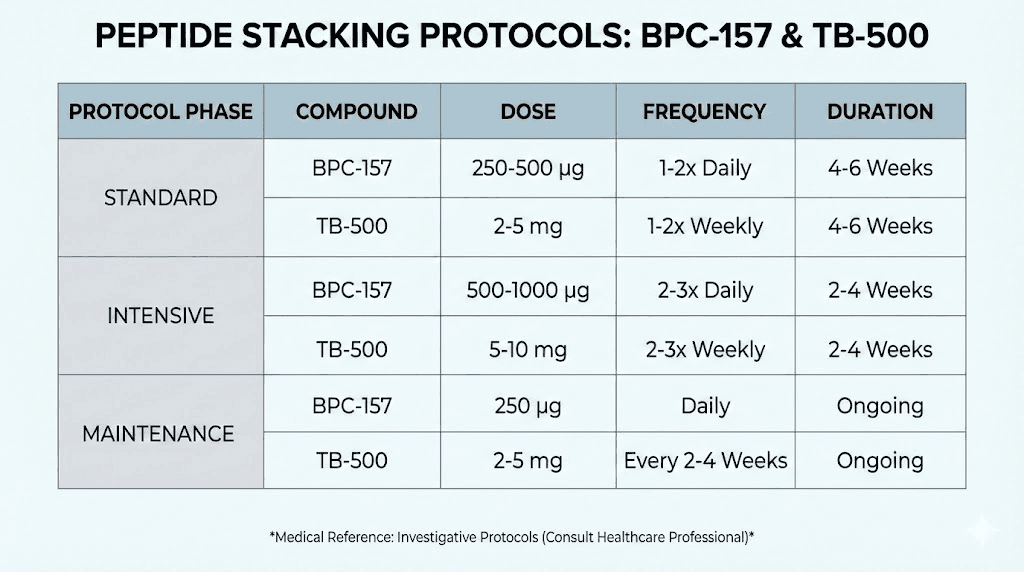
| Peptide | Typical frequency used in stacks | Common dose range people reference | When it’s usually adjusted |
|---|---|---|---|
| BPC-157 | Often daily during the active phase | Commonly referenced microgram-to-low-milligram range per day | If there’s no perceived effect after the early window, or if tolerance issues appear |
| TB-500 | Often several days apart during the active phase | Commonly referenced low dose per administration | If the user is aiming to extend duration or if recovery stalls |
Practical lesson from my hands-on planning: In real life, the biggest improvement comes less from “finding the perfect number” and more from starting consistent, tracking recovery markers, and not changing multiple variables at once. If you double doses and change training loading in the same week, you’ll never know what actually helped.
How to monitor whether the stack is helping
Use measurable, injury-specific indicators. I recommend tracking:
- Pain with a consistent movement (same angle, same load, same time of day)
- Range of motion (simple goniometer app or consistent photo angle)
- Function tests (e.g., sprint mechanics, step-down quality, grip endurance)
- Swelling/heat if relevant
- Sleep quality (recovery speed tracks strongly with sleep)
If you don’t see any shift at all after a reasonable adjustment window, that’s often a sign to re-check the fundamentals (load management, rehab consistency, and whether the diagnosis is accurate) rather than instantly escalating dosing.
Stacking schedule: timing, duration, and load management
In the stacking conversations online, people focus heavily on the dose. But from an outcomes standpoint, the interaction between dosing schedule and rehab loading often matters just as much.
My preferred planning approach
I plan around a recovery “loop”:
- Stabilize symptoms first: reduce aggravating load until baseline improves.
- Introduce rehab gradually: consistent mobility + targeted strength.
- Keep dosing consistent: avoid frequent micro-adjustments.
- Progress only one variable per week: either training load or exercise difficulty, not both.
Duration: how people commonly structure it
Most stack protocols are run for a defined window long enough to see early changes, then assessed. Users commonly report that early improvements (if any) show up before full tissue remodeling is complete, which is why “stacking duration” and follow-up rehab matter.
If you’re considering stacking for an accelerated healing goal, plan to treat the protocol as an assistance period for your rehab—not a replacement for it.
Safety, limitations, and quality control (what I’d watch for)
Because products in the peptide market vary in handling, purity, and labeling, real-world risk is often driven by the source and preparation quality, not just the concept of stacking.
Quality and contamination risk
- Verify storage practices (peptides typically require careful handling).
- Ensure reconstitution guidance is followed precisely (mis-handling can affect concentration).
- Be cautious if products lack clear batch documentation.
Individual variability
Even when people use similar dosing schedules, responses differ. In practice, I’ve seen the same protocol produce different outcomes depending on injury severity, time since injury, and whether the person actually managed mechanical load appropriately.
When you should not “push through”
If you have escalating pain, worsening range of motion, signs of infection/inflammation at injection sites, numbness/tingling, or symptoms that don’t fit the expected healing pattern, stop and seek medical guidance. The goal is recovery, not prolonged experimentation.
How to choose a stacking approach for your situation
Not every injury responds the same way to the same plan. Here’s a practical way to choose a stacking strategy.
More likely to fit a “stack-assisted rehab” mindset
- Soft-tissue injuries where rehab is already improving symptoms
- Recovery that feels slow after the early acute phase
- Cases where you can commit to consistent physical therapy-style work
Less likely to be solved by stacking alone
- Injuries with unclear diagnosis or suspected structural damage needing evaluation
- Situations where sleep, nutrition, and training load management are not under control
- Where the injury keeps getting re-aggravated by daily activities or training
Product image
FAQ
What is the recommended dose of BPC-157 and TB-500 for stacking?
There isn’t one universal recommended dose. Community protocols typically use a more frequent daily schedule for BPC-157 and a less frequent administration pattern for TB-500, with microgram-to-low-milligram ranges referenced online. The best approach is to start conservatively within common ranges, keep dosing consistent, and adjust only one variable at a time based on measurable recovery markers.
How long should I run a BPC-157 TB-500 stack?
Most people run a defined active window and then reassess based on pain, range of motion, and functional performance. If symptoms improve, continue the rehab progression alongside the protocol; if there’s no meaningful change, it’s usually smarter to reassess diagnosis, rehab loading, and fundamentals rather than immediately increasing the dose.
Is stacking better than using only one peptide?
Sometimes people report better outcomes with a combined stack, but it’s not guaranteed. In my experience, many “success stories” are driven by consistent rehab and load management more than the addition of a second peptide. If you’re new, a practical method is to start with a single peptide approach long enough to evaluate response before stacking.
Conclusion: A smart stacking plan beats guesswork
BPC-157 TB-500 stacking is popular because it offers a structured way to support recovery, and people often believe the two peptides complement each other. But the real leverage comes from combining dosing consistency with measurable progress tracking and responsible rehab loading. If you want to use a recommended dose of bpc 157 and tb 500 approach, treat dosing as just one part of a bigger recovery system—then adjust thoughtfully based on outcomes, not online pressure.
Next step: Pick one stacking template, choose a conservative starting plan, and begin a 7–14 day tracking routine (pain score on one movement, range of motion, and one function test) while you follow a consistent, rehab-focused training load.
Discussion