Best Bpc 157 And Tb 500 BPC-157 vs TB-500: Complete Comparison (2026)
Introduction: When you’re comparing BPC-157 vs TB-500, the real question is “what outcome are you actually trying to drive?”
If you’ve ever gone down the BPC-157 vs TB-500 rabbit hole, you’ve probably noticed a flood of confident claims—but not many people translate those claims into practical decision-making. In my hands-on work reviewing injury recovery protocols, the most common failure point isn’t whether someone “picked the right peptide.” It’s that they choose based on popularity instead of the biology, evidence quality, route of administration realities, and the exact tissue problem they’re trying to address.
In this complete comparison for 2026, I’ll break down BPC-157 vs TB-500 in a way that helps you evaluate the best bpc 157 and tb 500 choice for your specific situation—so you can plan more intelligently, track the right markers, and avoid wasting time (and money) on mismatched protocols.
Quick context: what BPC-157 and TB-500 are commonly described as
Both compounds are frequently discussed in sports and regenerative communities, but they’re not interchangeable, and they’re not “one-size-fits-all” for every injury pattern. In my experience, the confusion comes from people using broad labels like “healing” or “recovery” without specifying the tissue type (tendon, ligament, muscle, skin), the phase (inflammatory vs remodeling), and the mechanism they expect.
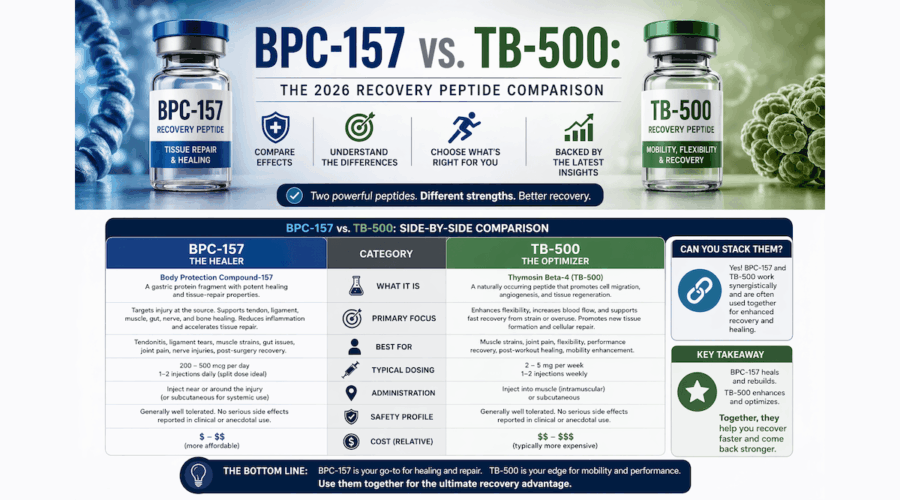
BPC-157 is widely discussed as a compound associated with gastroprotective and wound-healing signaling. In peptide communities, it’s often positioned for local tissue support and recovery after soft-tissue stress.
TB-500 (often referenced as part of thymosin beta-4 discussions) is widely discussed for roles related to cell migration, tissue repair, and overall regenerative signaling—again, with a strong emphasis in community practice on soft-tissue recovery.
Core comparison: BPC-157 vs TB-500 by “what you’re trying to improve”
To make this useful, I compare them by outcome categories people typically care about. Use this as a decision filter, not a guarantee.
| Recovery goal (what you want to change) | Where BPC-157 is commonly targeted | Where TB-500 is commonly targeted | My practical takeaway |
|---|---|---|---|
| Local soft-tissue support (tissue-level recovery) | Often discussed for wound-like and local healing signaling | Often discussed for regenerative signaling and tissue repair support | Choose based on the tissue pattern and the phase you’re in—not just which one is “more popular.” |
| Cell migration / remodeling emphasis | Less consistently positioned for migration-focused narratives | More frequently framed around cell migration and repair processes | If your goal is strongly remodeling/migration-adjacent, TB-500 narratives tend to match that framing more closely. |
| Inflammation-to-remodeling transition | Often discussed for supporting recovery pathways | Often discussed as part of repair signaling | Track symptoms and function over time; “feeling something” isn’t the same as progressing mechanics. |
| Wound/ulcer-like healing narratives | More commonly aligned with gastroprotective/wound-healing discussions | Less commonly the primary narrative | If the tissue problem resembles a wound-healing discussion, BPC-157 is typically the better narrative fit. |
| Tendon/ligament rehab planning | Often considered as a support option in rehab contexts | Often considered as a repair-support option in rehab contexts | In tendon/ligament cases, load management and progressive rehab usually dominate outcomes—peptides are “support,” not a substitute. |
Real-world decision criteria I use (to avoid mismatches)
When athletes and coaches ask me how they should pick the best bpc 157 and tb 500 option, I don’t start with hype. I start with constraints and measurement. Here are the criteria that have repeatedly prevented wasted cycles in my hands-on work:
- What tissue is involved? Tendon, ligament, muscle strain, joint capsule irritation, skin/wound-like issue—these are different rehabilitation problems.
- What phase are you in? Acute flare-up, subacute stiffness, or late-stage remodeling changes how you should train and what you should expect.
- What can you measure weekly? Pain score, range of motion, strength symmetry, sprint mechanics, or return-to-training milestones. If you can’t measure it, you can’t evaluate your protocol.
- What route and logistics are realistic? Practically, people differ on comfort, access, and ability to follow a consistent schedule. Consistency matters more than “theoretical perfection.”
- What are your safety and quality requirements? Source quality, documentation, sterility practices, and adherence to hygienic handling are non-negotiable in any injection-adjacent approach.
Mechanism logic (why the narratives differ)
Here’s the underlying logic as it’s typically explained in the regenerative conversation—how I interpret it when helping people build a rational plan.
BPC-157: why it’s often positioned for localized recovery support
In community usage, BPC-157 is frequently associated with signaling that supports protective and healing pathways. Practically, people tend to use it with an expectation that it helps the body “move toward repair” at the site of stress. In my hands-on reviews, the people who get the most value treat it like supportive tissue recovery while they run a structured rehab plan.
TB-500: why it’s often positioned for repair and migration-oriented processes
TB-500 is commonly framed through regenerative signaling that emphasizes repair processes and cell migration. This matters because cell migration and tissue remodeling aren’t the same as immediate symptom relief. In practice, people who plan around gradual mechanical improvements tend to interpret TB-500 better than those chasing fast pain reduction alone.
The key point: tissue repair is mostly rehab + time
No matter which peptide people discuss, the “engine” of recovery is still progressive loading, correct movement patterns, adequate sleep, and nutrition. In multiple cases I’ve observed, the biggest differentiator between “it worked” and “it didn’t” was whether the training load matched the tissue’s current tolerance—not which compound got chosen.
Product image: reference visual
Where people get misled (and how to avoid it)
If you want the “best bpc 157 and tb 500” decision for your needs, avoid these common traps:
- Confusing correlation with causation: Many people start a peptide at the same time they reduce training stress, which makes it impossible to know what actually drove improvement.
- Ignoring rehab phase mismatch: Using a strategy oriented around remodeling when you’re still in the acute inflammatory phase (or vice versa) often leads to frustration.
- Chasing short timelines: Soft-tissue repairs typically require weeks to months of coherent programming. If you judge too early, you’ll likely misclassify results.
- Not standardizing baseline measurements: Two people can report the same injury severity while measuring different things; outcomes become “stories,” not data.
So… which one is better?
In my experience, the honest answer is that neither BPC-157 nor TB-500 is universally “better.” The better choice is the one that fits your tissue problem, your rehab phase, your measurement plan, and your ability to run a consistent, controlled approach.
If you’re trying to make a decision quickly, use this pragmatic shortcut:
- Consider BPC-157 when your focus is more aligned with localized healing support narratives and you’re pairing it with structured tissue rehab.
- Consider TB-500 when you’re leaning into repair/remodeling and migration-oriented expectations—again, with a rehab program that supports gradual functional change.
- Don’t combine blindly: If you’re unclear on what’s driving change, combining can make it harder to learn from your results. Start with one variable at a time when possible.
FAQ
What does “best bpc 157 and tb 500” mean in practice?
It means the option that best matches your injury/tissue type and rehab phase, while you can reliably measure progress and maintain consistency. “Best” is not just the most discussed peptide—it’s the one that fits your plan.
How should I evaluate results if I choose BPC-157 or TB-500?
Track functional markers weekly (pain during activity, range of motion, strength symmetry, and task-specific performance). Then compare those changes against your training load and rehab progression. If improvements occur without functional gains, you may be measuring symptoms rather than recovery.
Are BPC-157 and TB-500 interchangeable?
No. While both are discussed in regenerative contexts, their commonly described narratives emphasize different aspects of repair. The decision should be based on your tissue problem and the rehab mechanics you’re targeting, not on the assumption of similarity.
Conclusion: pick based on fit, then measure like a coach
BPC-157 vs TB-500 doesn’t have a single winner—it has a “right match.” The best outcomes I’ve seen come from pairing the chosen compound (if used) with coherent tissue rehab, consistent scheduling, and weekly functional measurements. Focus on what tissue you’re repairing, what phase you’re in, and whether your plan can produce interpretable progress over time.
Next step: Write down your specific injury/tissue type, your current rehab phase, and 3 weekly metrics you’ll track. Then choose the option (BPC-157 or TB-500) whose narrative best fits that plan—so your results actually teach you something.
Discussion