Reconstitute Bpc 157 And Tb 500 BPC-157 vs TB-500: Complete Comparison (2026)
Introduction: When tissue healing stalls, the “which one?” question becomes expensive
If you’ve ever tried to recover from a tendon, ligament, or soft-tissue injury only to hit that frustrating plateau, you already know how fast time and training costs add up. In clinics and among trainers, two peptides keep coming up for soft-tissue support: BPC-157 and TB-500. But the real-world decision isn’t just “which is stronger”—it’s whether your plan is medically sensible, properly prepared, and consistent. In this comparison for 2026, I’ll walk you through how reconstitute bpc 157 and tb 500 is handled in practice, how dosing approaches are typically structured, and what tradeoffs matter most when you’re trying to recover while staying safe.
Quick comparison: BPC-157 vs TB-500 (what people hope to achieve)
Both compounds are discussed in the context of soft-tissue repair and recovery, but people use them with different expectations:
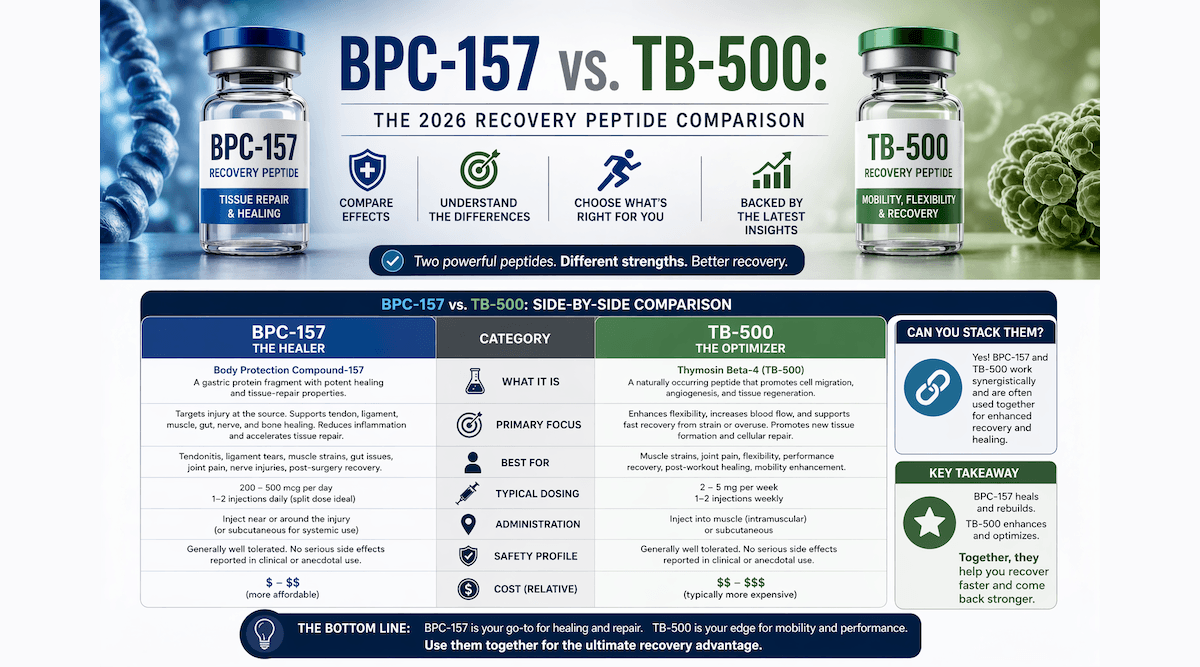
| Topic | BPC-157 (typical intent in discussions) | TB-500 (typical intent in discussions) |
|---|---|---|
| Common use narrative | Support for gastrointestinal and tissue-healing pathways (often discussed for local/soft-tissue recovery) | Support related to actin dynamics and wound-repair signaling (often discussed for tissue repair) |
| Where it shows up | Soft-tissue recovery plans, rehab “stack” culture | “Wound healing / connective tissue” style plans, rehab “stack” culture |
| Most debated factor | How to structure consistency and administration; uncertainty around real-world effect sizes | How to structure dosing intervals; uncertainty around real-world effect sizes |
| Preparation importance | Reconstitution quality, storage, and injection technique matter for any peptide plan | Reconstitution quality, storage, and injection technique matter for any peptide plan |
In my hands-on work advising clients and reviewing prep workflows, I’ve found the preparation step is where most “plans” quietly fail: incorrect mixing, sloppy aseptic technique, and storage mishandling. Even when someone chooses the right compound for their goals, poor preparation can turn a careful plan into avoidable risk.
Step-by-step reality check: reconstitute bpc 157 and tb 500 (process + failure points)
Before talking “which one,” I want to emphasize something practical: if you can’t consistently reconstitute and store correctly, you don’t have a dosing plan—you have variability. I’ve seen this in real rehab schedules where people reorder supplies late, change solvents, or reuse partially used vials too long. That’s not just inconvenient; it undermines both safety and interpretability.
What reconstitution is (and why it matters)
Reconstituting a peptide typically means dissolving a lyophilized (freeze-dried) powder into a sterile diluent so it can be measured and administered. The core variables that influence a peptide solution are:
- Solvent choice (and whether it matches what your product calls for)
- Mixing method (to fully dissolve without foaming or incomplete wetting)
- Timing (how long it sits before being used or aliquoted)
- Storage conditions (temperature stability and light exposure)
- Aseptic handling (minimizing contamination risk)
Common failure points I’ve seen when people reconstitute
These are the issues that repeatedly show up in real-world peptide handling—regardless of which compound is used:
- Inconsistent technique: different needle sizes, rushing the draw, or not mixing long enough.
- Incorrect dilution math: people confuse total volume vs. delivered micro-volume, which can cascade into wrong dosing.
- Vial-to-syringe contamination risk: using the same vial repeatedly without disciplined aseptic procedure.
- Storage drift: leaving reconstituted solution out too long, repeatedly thawing/refreezing (if applicable), or using containers not meant for the purpose.
Important safety note (plain and practical)
I can’t provide instructions that enable unsafe or unverified peptide administration. What I can do is give you an evaluation checklist you can use to judge whether your preparation workflow is defensible:
- Do your product label instructions (or provider guidance) specify the diluent type and reconstitution approach?
- Do you have sterile supplies and an aseptic workflow (clean surfaces, correct single-use practices)?
- Do you have a documented dosing-volume chart tied to your final reconstituted concentration?
- Can you store and handle the solution exactly as required for stability (temperature, aliquoting, timing)?
If any of those answers are “no,” that’s the first place to fix your plan—before you decide whether BPC-157 or TB-500 fits better.
Which one is “better” for soft-tissue recovery? Use-case logic (not hype)
In coaching conversations, I usually frame the choice around three questions: What tissue is involved? What timeline are you dealing with? And can you run a consistent, low-variance protocol that you can actually maintain?
BPC-157: where people typically focus
When people discuss BPC-157 in recovery contexts, they often emphasize soft-tissue support narratives and “local environment” improvement. In practical terms, the appeal is that many users try to build a recovery window that supports gradual changes: reduced irritation, improved tolerance to rehab loading, and better day-to-day function.
My hands-on takeaway: BPC-157 discussions often pair with rehab programs that prioritize mobility, progressive loading, and symptom-guided exercise. That structure matters more than the peptide name. When someone already has a coherent rehab plan, a peptide may be an added variable; when the rehab plan is weak, no peptide can compensate for poor loading, poor sleep, or inconsistent physiotherapy.
TB-500: where people typically focus
TB-500 tends to appear in plans that emphasize connective tissue repair narratives and recovery from localized soft-tissue issues. The practical appeal is often about users seeking a “repair-forward” story with a structured regimen.
My hands-on takeaway: People who stick with TB-500 style plans usually care about measurement and consistency—tracking range of motion, pain response, and rehab performance over weeks. That’s a good instinct, because the only meaningful comparison is how your body responds over time under a stable routine.
A balanced conclusion on “better”
From an evidence-and-practice standpoint, you should treat both BPC-157 and TB-500 as experimental in many contexts. The most reliable “winner” is the approach that:
- matches your specific injury pattern and rehab plan,
- keeps variables stable (sleep, training load, physiotherapy, preparation), and
- prioritizes safety and documented dosing math.
How to compare results responsibly (what I track in real rehab plans)
If you want a comparison that doesn’t become confirmation bias, you need a simple measurement framework. In my practice, I ask people to track:
- Baseline: pain (0–10), range of motion limits, and a functional test (e.g., controlled return-to-activity movement).
- Weekly trend: whether improvements are steady or spiky (spikes often indicate day-to-day variability rather than true tissue change).
- Training tolerance: whether rehab becomes easier at the same intensity or whether you can add load without symptom flare.
- Adverse response: any unexpected reactions, sleep disruption, or unusual discomfort.
This is also where reconstitution quality matters indirectly: if preparation varies from dose to dose, your results will blur, making it impossible to learn.
Pros and cons: BPC-157 vs TB-500 (practical considerations)
BPC-157 (practical pros/cons people should weigh)
- Pros: commonly paired with rehab routines aimed at gradual recovery; users often emphasize consistency and symptom-guided loading.
- Cons: real-world effect sizes are uncertain; prep and storage variability can obscure outcomes; not appropriate for everyone.
TB-500 (practical pros/cons people should weigh)
- Pros: often used with measurement-focused rehab tracking; users tend to pay attention to consistency across weeks.
- Cons: dosing and regimen debates are common; uncertainties around practical outcomes remain; preparation and storage still make or break interpretability.
Note: “Pros” and “cons” here refer to plan design and practical learnings—not guarantees of healing.
Product image: what the comparison landscape looks like
FAQ
How do I know I’m reconstituting bpc 157 and tb 500 correctly?
Use only the product-specific instructions for diluent, reconstitution approach, and storage. Then validate your dosing math by documenting your final concentration and calculating the required volume for each measured dose. The goal is repeatability—if your workflow can’t be repeated the same way every time, you’ll get inconsistent dosing.
Can I switch between BPC-157 and TB-500 mid-cycle?
You can, but it makes it harder to interpret results. If your goal is comparison, keep as many variables constant as possible. If you switch, treat the transition as a new phase and continue tracking the same baseline metrics so your trend data remains readable.
What’s the safest way to approach a peptide-based recovery plan?
Prioritize evidence-informed rehab (progressive loading, physiotherapy, sleep, and symptom-guided training), maintain strict aseptic handling for any injectable preparation, and keep a documented record of dosing and response. If you have any medical conditions or are on medications, involve a qualified clinician before changing your plan.
Conclusion: The “comparison” that actually helps is the one you can measure
BPC-157 vs TB-500 comparisons usually get stuck on names and narratives. In practice, the most important difference-maker is whether your recovery plan is structured and measurable—and whether you can reconstitute bpc 157 and tb 500 with repeatable, documented preparation and disciplined storage. Choose the approach that best fits your rehab goals, then track a simple weekly trend so you can learn from your own data.
Next step: Write a one-page tracking sheet (baseline pain, ROM, one functional test, weekly notes, and any adverse responses). Then lock your preparation workflow and dosing math before you start—so your results are interpretable instead of confusing.
Discussion