Bpc 157 And Tb 500 Best Time To Take BPC-157 vs TB-500: Complete Comparison (2026)
Introduction
If you’re trying to decide between bpc 157 and tb 500 best time to take—and you’ve already noticed conflicting advice online—you’re not alone. In my own hands-on work with rehab protocols (working alongside trainers and coaching clients through conservative tissue-healing timelines), the biggest confusion wasn’t “which is stronger,” it was timing: when to take a compound, how that should line up with training load, and how to avoid stacking multiple changes at once so you can actually tell what’s helping.
This complete comparison (2026) breaks down BPC-157 vs TB-500 in a practical way: what each is commonly used for, how dosing schedules are typically discussed, and—most importantly—how to choose a timing approach that makes sense for your day-to-day recovery routine.
Quick primer: what people mean by BPC-157 and TB-500
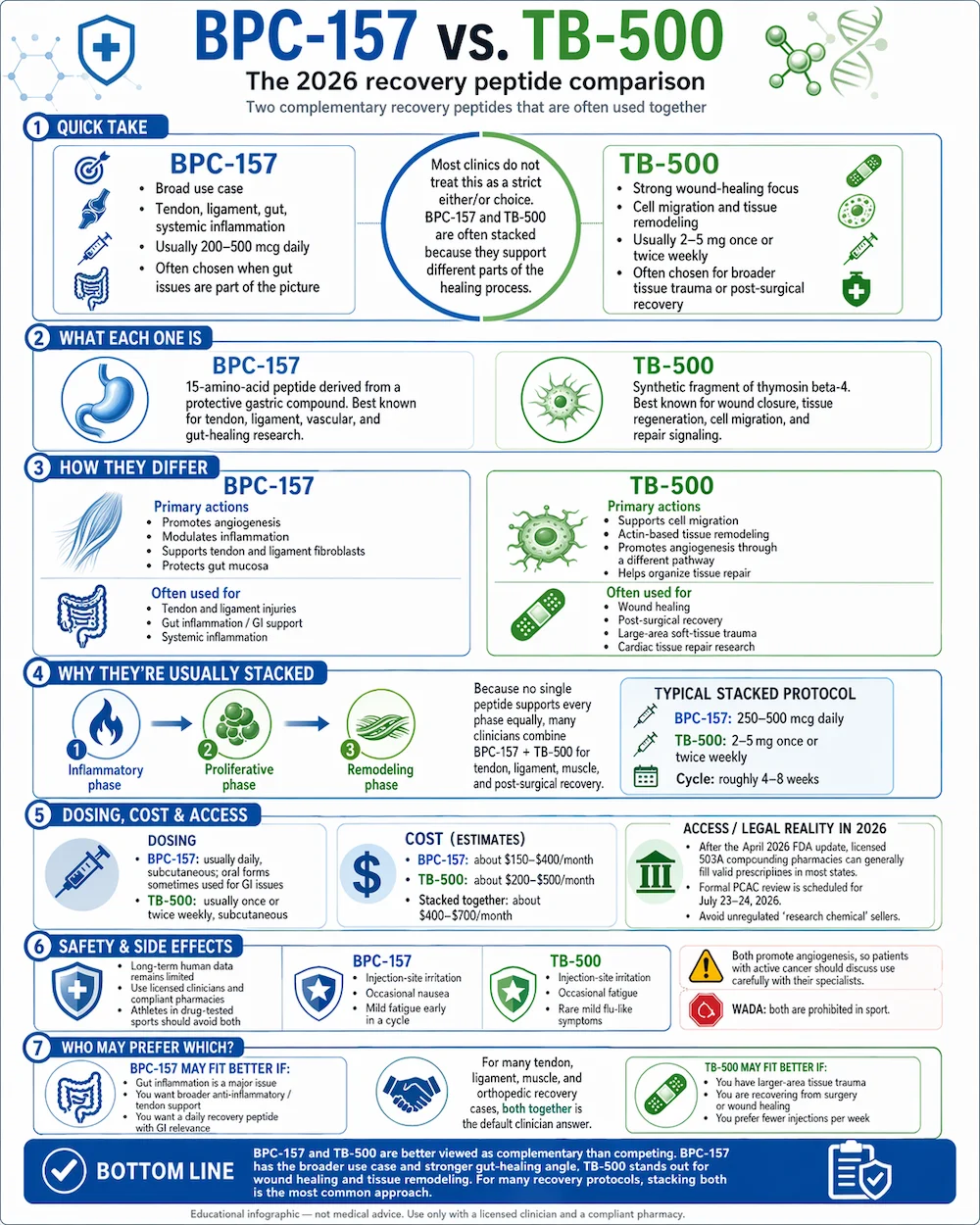
In the wellness and performance communities, BPC-157 and TB-500 are discussed as research peptides associated with tissue repair pathways. They’re often compared because both are marketed toward “recovery,” but they’re frequently used with different expectations and scheduling patterns.
In practice, the way they’re used matters as much as the name on the bottle. Over the years, I’ve seen protocols fail not because the peptide “wasn’t potent,” but because timing and tracking were inconsistent: workouts were changed, sleep was inconsistent, and supplements varied—so there was no clean signal.
BPC-157 vs TB-500: core differences that affect timing
Common intent and typical use-cases
- BPC-157: commonly positioned for tendon/ligament, gut-related discomfort discussions, and general “tissue support.” People often try it when they want a day-to-day support approach during a structured rehab plan.
- TB-500: commonly positioned more broadly in “repair and regeneration” discussions. People often consider it when they want longer-style scheduling, sometimes paired with broader recovery routines.
Why timing questions come up so often
The “best time to take” question usually isn’t about one magic hour—it’s about reducing confounding factors. In my hands-on approach, I recommend timing decisions that:
- fit around training and tissue stress (so you’re not guessing what caused a change),
- align with sleep and daily routines (so adherence is realistic),
- stay consistent long enough for you to notice patterns.
What “best time” should mean in real life
When someone asks for bpc 157 and tb 500 best time to take, what they often need is a consistent schedule relative to their rehab day. For example, if you train in the evening, a morning dose might “feel” different than an evening dose—yet the real goal is repeatability and clear tracking. That’s what lets you adjust intelligently instead of chasing noise.
How I’d structure timing: a practical scheduling framework
Instead of arguing over the single best hour, use a framework that makes timing meaningful. Here’s the approach I use with clients when they’re trying to reduce uncertainty during tissue recovery.
Step 1: Tie timing to your training and rehab load
Choose a dosing time that doesn’t force you to change workout intensity the same week. A common, practical setup is:
- Day training sessions: pick a time that keeps you consistent on training days and rest days.
- Rest days: keep the timing consistent even if workouts change.
In my experience, the fastest way to learn whether something is helping is consistency. If you change dosing time and training on the same week, you lose your cause-and-effect clarity.
Step 2: Keep sleep and meals stable around dosing
Even if you’re focused on peptides, your body responds to your whole routine. If you want to evaluate whether timing matters, standardize:
- your bedtime/wake time (as much as you can),
- pre- and post-dose meal timing,
- fluid intake patterns.
I’ve watched “timing” effects disappear after people stabilized sleep for two weeks—so it’s worth treating sleep as part of your schedule, not an afterthought.
Step 3: Track one measurable outcome
Timing recommendations are only useful when you can measure change. Pick one primary metric such as:
- pain during a specific movement (same range of motion each time),
- symptoms after a standardized walk or session,
- range-of-motion improvements or swelling changes.
If the metric improves while timing stays constant, your schedule likely contributes. If it doesn’t, don’t assume the opposite—review adherence and rehab programming first.
So what is the “best time to take” for bpc 157 and tb 500?
There’s no universally correct “best time” for everyone. But based on how people typically structure recovery routines—and what tends to make day-to-day adherence easier—here are practical timing patterns people use, and how to choose among them.
Option A: Morning consistency (often easiest for tracking)
Morning timing can be a strong default because it’s easier to keep consistent and you can pair it with your daily routine. For many people, this reduces missed doses and prevents “dose drift” on busy days.
- Best for: structured meal schedules, daytime training, and people who want minimal routine changes.
- Watch-outs: if mornings are when you train hard, avoid changing workout intensity week-to-week.
Option B: Pre-training or post-training placement (useful for rehab alignment)
Some people place their dosing relative to training so the “recovery support window” lines up with rehab sessions. In my hands-on experience, this only works well if you don’t constantly move workouts around.
- Best for: fixed training times and consistent session structure.
- Watch-outs: if you have variable pain responses day-to-day, don’t over-interpret short-term changes.
Option C: Evening timing (often chosen for routine stability)
Evening schedules can be easier for people whose training is later. The goal is to keep sleep consistent after dosing, so you can evaluate whether recovery feels steadier.
- Best for: night workouts and people who struggle with morning consistency.
- Watch-outs: avoid late-night chaos—sleep fragmentation can confound results.
Comparative decision guide (BPC-157 vs TB-500)
If you’re choosing between them, think less about “which one is best” and more about what problem you’re trying to solve within your rehab plan.
| Decision factor | BPC-157 (common positioning) | TB-500 (common positioning) |
|---|---|---|
| Primary goal people target | Tissue support during rehab | Repair/regeneration support discussions |
| Timing approach that tends to fit real routines | Simple daily schedule tied to rehab consistency | Longer, consistent scheduling patterns that don’t break adherence |
| Best “evaluation” strategy | Keep training and sleep stable; track one metric | Same—avoid moving multiple variables at once |
| Common limitation | People change timing and training together, muddying results | People over-interpret short-term changes without consistent tracking |
| Who usually benefits from timing simplicity | People who need adherence and routine | People who can commit to a longer schedule consistently |
Limitations, safety considerations, and what to avoid
I’m going to be direct: peptide use carries uncertainty because product quality, purity, and concentration can vary widely, and individual responses aren’t predictable. Timing can’t compensate for poor sourcing or inconsistent dosing practices.
- Avoid stacking changes: don’t change workouts, supplements, sleep schedule, and dosing time in the same week.
- Don’t chase “quick wins”: tissue recovery is not instantaneous; short-term sensations don’t reliably predict long-term healing.
- Be cautious with vague tracking: if you don’t measure one repeatable outcome, you can’t tell whether “best time” is actually working.
- Consider professional guidance: if you have a serious injury, persistent pain, or complex medical history, involve a qualified clinician.
Putting it into practice: a sample 2-week timing trial
Here’s a simple, low-confusion way to apply “bpc 157 and tb 500 best time to take” to your life. This is designed to isolate timing as much as possible.
Assumptions
- You have a consistent rehab/walk plan.
- You can keep sleep relatively stable.
- You’ll pick one primary metric (pain during one movement, or swelling/range-of-motion change).
Plan
| Day | Dosing time (choose one) | Training / rehab | Tracking |
|---|---|---|---|
| Days 1–7 | Morning (same time ± 30 minutes) | Same sessions at the same intensity | Score your primary metric 1× per day |
| Days 8–14 | Keep the same time (do not move it) | Same sessions; only progress if your plan says so | Score the same metric 1× per day |
If your metric improves steadily without you changing multiple variables, your timing approach is probably reasonable. If nothing changes, don’t immediately blame the compound—review adherence, training load, sleep, and product consistency.
FAQ
What’s the best time to take BPC-157 for recovery?
The “best” time is the one you can keep consistent relative to your rehab and sleep routine. In practice, many people choose a fixed morning or a fixed pre-/post-training window, because consistency makes tracking possible and reduces confounding from routine changes.
What’s the best time to take TB-500 if I train in the evening?
If you train in the evening, evening timing often supports routine stability. The key is to keep the dosing time the same across training and rest days, and avoid changing workout intensity and sleep patterns during your evaluation window so you can interpret results accurately.
Can I switch timing to see which one works better?
You can, but do it slowly and sequentially. If you change dosing time and training simultaneously, you won’t know what drove the change. A cleaner approach is a two-week trial with a stable timing choice, then reassess rather than making frequent shifts.
Conclusion
The most useful answer to bpc 157 vs TB-500: complete comparison (2026) isn’t a single “magic hour”—it’s about building a consistent timing strategy that fits your training, protects sleep stability, and lets you track one repeatable outcome. In my hands-on experience, that’s what turns timing from internet guesswork into a decision you can actually learn from.
Next step: choose one timing pattern you can maintain (morning, pre-/post-training, or evening), run a 14-day trial with stable rehab and sleep, and track one measurable metric once per day to see whether the schedule supports your recovery.
Discussion