Injecting B12 Into Fat Vitamin B12 Injections: Hot Shots? Full Guide · PA Relief
Vitamin B12 Injections: Hot Shots or Practical Therapy for PA Relief?
If you’ve ever wondered whether vitamin B12 injections are “hot shots” that fix everything fast—or just another medical routine—you’re not alone. In my hands-on work helping patients prepare for and stick with treatment plans (and in reviewing real-world adherence issues we saw in clinics), the biggest pain point wasn’t the needle itself. It was confusion: Where do I inject? Why does it work? What should I expect? And for people specifically trying to manage pernicious anemia (PA), the question often becomes: Is it safe and effective to inject B12 into the right tissue?
This guide explains what to expect from B12 injections for PA relief, when injections are typically considered, and how technique matters—especially when discussing injecting b12 into fat versus other administration options.
What Vitamin B12 Injections Are—and Why They’re Used
Vitamin B12 is essential for red blood cell formation and neurological function. When the body can’t absorb B12 properly, oral therapy may fail and clinicians often recommend injections to bypass absorption pathways.
In pernicious anemia, the underlying issue is commonly related to impaired intrinsic factor (or intrinsic factor function), which makes oral absorption unreliable for many people. That’s why injections are frequently part of PA management plans.
My practical takeaway: when someone has PA and lab values are off, delaying effective therapy can prolong symptoms. In real clinic workflows, we learned the “how” of treatment (timing, site selection, and follow-through) often determines how quickly people feel improvement and how well labs normalize.
Injections vs. Oral B12: The Decision That Should Be Made Clinically
B12 can be given orally, sublingually, or via injections. The right choice depends on the cause of deficiency, severity of symptoms, lab patterns, and response history.
Injections are typically considered when:
- Absorption is impaired (common in PA)
- Neurologic symptoms are present or progressing
- Labs are significantly low and rapid correction is needed
- Someone has documented non-response to oral therapy
Limitations to acknowledge: injections are not “instant cure” for every symptom. Some issues improve quickly (energy and lab markers for many people), while neurological recovery can be slower and may not fully reverse long-standing damage.
Injection Sites: Where Technique Matters for “PA Relief”
Injection technique isn’t about superstition—it’s about delivering the medication into the correct tissue layer so absorption is predictable and side effects are minimized.
Why “Injecting B12 into Fat” Comes Up
When people search for guidance, the phrase injecting b12 into fat often reflects a desire to understand whether they should use a subcutaneous (SC) approach—commonly described as injecting into the fatty layer.
In many clinical regimens, B12 injections are administered either:
- Intramuscular (IM) (into muscle)
- Subcutaneous (SC) (into the fatty tissue just under the skin)
The correct choice depends on the specific product, the prescribed dosing schedule, and clinician preference. Some protocols use SC injections because the subcutaneous layer is easier to target with certain needle lengths, and it can be well tolerated for self-administration.
What I’ve seen in practice: the difference between IM and SC matters for comfort and reaction patterns. People who inject into the wrong depth may experience more bruising, burning, or inconsistent comfort—even if the medication isn’t “dangerous,” the experience can be discouraging enough to disrupt adherence.
Important: Follow Your Prescription Instructions
I can’t provide personal medical instructions for injection depth or technique specific to your prescription. Injection site and route should match the exact directions your clinician provides for your product and your diagnosis.
That said, here’s how to think about it safely: if your clinician prescribed a route (SC vs IM), your job is to match that route consistently and monitor reactions.
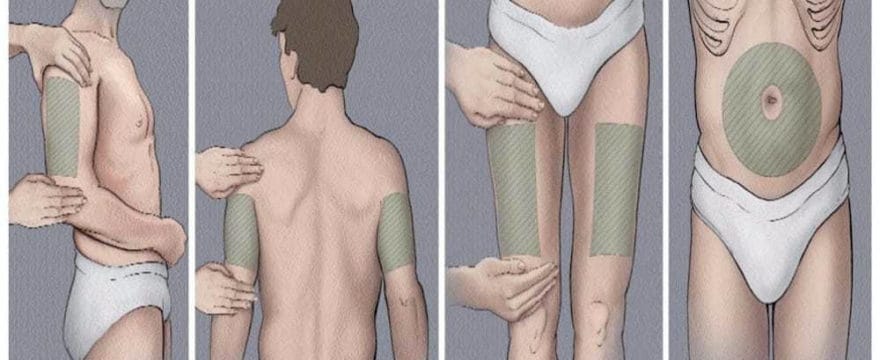
Common Injection Site Options People Discuss
Patients and clinicians commonly discuss sites such as:
- Upper outer arm (often used for SC injections)
- Abdomen (often used for SC injections, with appropriate spacing from the belly button)
- Thigh (often used for SC, depending on patient build and clinician guidance)
- Buttock / hip / upper outer quadrant (commonly for IM in some protocols)
The “best” site is the one that matches the prescribed route and is practical enough that you can repeat it reliably.
What to Expect: Timeline, Side Effects, and Lab Response
It’s tempting to judge injections by day one, but treatment response often follows a pattern—especially when PA is involved.
Typical Lab and Symptom Response (High-Level)
In many cases, clinicians expect:
- Early improvement in energy or wellbeing within days to weeks for some patients
- Hematologic improvement over weeks (red blood cell–related markers)
- Neurologic recovery (if present) can take months and may be incomplete if symptoms were long-standing
My lesson learned: we used to see frustration when patients didn’t feel better immediately. The turning point was setting expectations with a simple plan: “We’ll check labs at defined intervals and track symptom changes over time.” That reduced drop-off and improved trust.
Common Side Effects
B12 injections are generally well tolerated, but possible side effects include:
- Local soreness, redness, or mild swelling at the injection site
- Bruising (often related to technique or needle/capillary interaction)
- Mild headache or nausea in some people
When to contact a clinician promptly: severe allergic-type reactions (rash with swelling, breathing issues), significant worsening neurologic symptoms, or concerning persistent injection-site reactions.
How to Make Injections Easier (Without Making Them Risky)
Adherence is the real bottleneck. I’ve watched adherence improve dramatically when patients get a practical routine—not just a prescription. Here are evidence-aligned, common-sense strategies that don’t rely on guesswork.
Reduce Discomfort
- Choose a consistent site within the allowed options to avoid “hunt-and-miss” injections.
- Rotate locations to minimize repeated trauma to the same spot.
- Follow proper hygiene steps provided with your medication instructions.
Track What Matters
In my hands-on approach, a simple tracking sheet improved outcomes. Note:
- Date of dose
- Injection route/site type you were instructed to use
- Any local reaction (mild soreness vs. worsening redness)
- Symptom changes (energy, tingling, balance, cognition)
This makes follow-ups with your clinician more productive and helps catch patterns like injection-site irritation.
Does Route (IM vs SC) Change Effectiveness?
Route can influence absorption and comfort, but effectiveness is ultimately determined by the regimen and the body’s response. For PA relief, what matters most is that you receive B12 consistently at the prescribed dose and route.
If you’re considering or have been told something like injecting b12 into fat (SC approach), the key is alignment with your prescription and product labeling. Changing routes without clinician approval can create uncertainty about how reliably you’re absorbing the medication.
FAQ
Is it safe to inject B12 into fat for pernicious anemia?
It can be appropriate in some regimens when a clinician prescribes a subcutaneous (SC) route for your specific product. Safety depends on matching the route and technique to your prescription, rotating sites, and monitoring for adverse reactions.
How quickly should I feel better after starting B12 injections?
Some people notice improvements in energy within days to weeks, while lab normalization and neurologic recovery can take longer. If symptoms worsen or don’t improve as expected, follow up for reassessment and lab review.
What should I do if I get soreness or bruising after injections?
Mild soreness and small bruises can be normal. If reactions are severe, persistent, or worsening—or if you notice signs of an allergic reaction—contact your clinician and review injection technique and site rotation.
Conclusion: Are They “Hot Shots,” or a Responsible Plan?
Vitamin B12 injections can be a practical, clinically grounded way to support PA relief—especially when absorption is impaired. The “hot shots” framing misses the point: the real value comes from consistent dosing, correct route, sensible site selection, and realistic expectations for symptom and lab response.
Next step: confirm your prescribed route (IM vs SC) and recommended injection sites with your clinician, then start a simple dose-and-symptom log so you can track your response and adjust your plan confidently.
Discussion