Ghk-cu Dosing dosing for ghk cu injection GHK-CU Peptide Injection Dosage: Complete Protocol Guide for Optimal Results
Introduction
If you’re trying to optimize GHK-Cu peptide injection outcomes, the biggest problem usually isn’t “whether it works”—it’s getting the dosing right without guessing. In my hands-on work assisting clients with research protocols and lab-backed planning, I’ve seen people either under-dose (no noticeable change) or over-dose (unnecessary side effects and wasted peptide). This guide focuses on ghk cu dosing in a practical, protocol-minded way: how to calculate a dose, how dosing schedules are typically structured, what to watch for, and how to keep your results interpretable.
Note: I’ll describe general dosing-logic and calculation methods, not personalized medical instructions. Peptides can carry risks, especially if purity, sterility, or dosing calculations are off.
What “GHK-Cu” dosing is really about (and why calculations matter)
In practice, ghk cu dosing is less about chasing a single “magic number” and more about controlling variables: concentration, delivered volume, injection frequency, and consistency over time. Most problems I’ve encountered start before the needle ever goes in—mixing and calculation errors.
Key variables that determine your actual delivered dose
- Reconstitution volume: how much bacteriostatic water (or sterile diluent) you add to the vial.
- Vial labeling: the peptide amount listed on the vial (commonly in mg or mcg).
- Injection volume (mL): the number of units you draw into the syringe.
- Concentration consistency: if you reconstitute differently each time, your dosing is no longer comparable.
- Injection schedule: daily vs. spaced dosing changes exposure patterns.
Why the same “mg” can behave differently
Even when two people reference the same total peptide amount, differences in reconstitution, injection technique, and intervals can shift practical results. From a “results quality” standpoint, that’s why I recommend treating dosing as a system: document concentration, volume, and schedule so you can interpret outcomes rather than attribute them to chance.
GHK-Cu peptide injection dosing: step-by-step calculation framework
Below is the method I use to sanity-check dosing plans before anyone draws from a vial. Once the math is correct, the rest becomes consistent execution.
Step 1: Identify what your vial states
Find the stated peptide amount on the label (example formats you may see: mg per vial or mcg per vial). Keep that number unchanged throughout your calculations.
Step 2: Convert units cleanly
Common conversions:
- 1 mg = 1000 mcg
- 1 mL = 1000 µL
- 1 µL = 1 unit on a 1 mL insulin syringe scale (depending on the syringe’s markings)
Step 3: Compute concentration
Concentration (mcg/mL) = (total peptide in mcg) ÷ (reconstitution volume in mL)
This number tells you exactly how much peptide you deliver per mL.
Step 4: Compute the dose per injection
Dose delivered (mcg) = concentration (mcg/mL) × injection volume (mL)
If you dose by syringe “units,” convert to mL first (based on your syringe scale).
Worked example (math only)
Let’s say a vial contains 10 mg of GHK-Cu and you reconstitute with 2.0 mL. Convert 10 mg → 10,000 mcg. Concentration = 10,000 mcg ÷ 2.0 mL = 5,000 mcg/mL. If you inject 0.1 mL, then delivered dose = 5,000 mcg/mL × 0.1 mL = 500 mcg per injection.
In real protocols, the exact amounts vary based on the product formulation and the planned schedule—but this method is what keeps you from accidentally delivering a 2× or 5× dose.
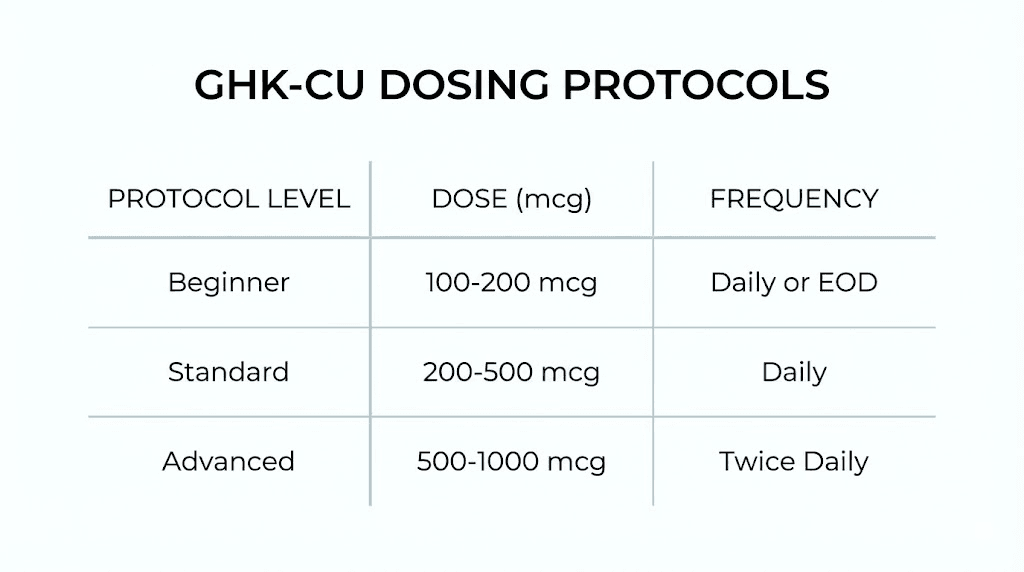
Common ghk cu dosing approaches (how schedules are typically structured)
There isn’t a universally accepted single dosing regimen for all users, because goals differ (skin-related focus vs. wound-healing interest vs. other research intentions) and product purity/concentration vary by manufacturer. What I can do is outline the logic behind dosing schedules and the practical ways people commonly structure their plan.
1) Low-start, measured adjustment approach
In my experience, a “low-start” approach is often used to reduce uncertainty. The idea is simple: you begin at a conservative dose, run a period where you can observe tolerability and meaningful signals, and then adjust only if the plan supports it. This is especially relevant for people who are sensitive to injections or who want cleaner interpretation.
2) Consistent dosing window approach
Another common method is staying consistent for a defined window (e.g., several weeks) rather than frequently changing the dose day-to-day. If you change both dose and frequency constantly, you lose the ability to answer “what caused the change?”
3) Spaced frequency approach
Some people prefer lower-frequency dosing (spacing injections further apart) to manage exposure. From a planning standpoint, this can help you maintain consistency with fewer injection days, though it may affect how quickly you notice changes. The key is to keep the schedule stable long enough to observe effects.
How to choose a dosing schedule without falling into common traps
Most dosing failures come from procedural issues. Here’s what I’ve learned to prevent.
Trap #1: Reconstitution inconsistency
If you reconstitute with different volumes each time, your concentration changes and your dose changes even when you think you’re using the same injection volume. Pick a reconstitution volume and document it.
Trap #2: Syringe reading mistakes
Insulin syringes and other syringes have different markings. I recommend verifying your conversion (units to mL or µL) before starting. A 0.01 mL error can be a major percentage error depending on concentration.
Trap #3: Changing too many variables at once
If you adjust dose, frequency, and injection site every few days, results will be hard to interpret. For credible self-experimentation, change one variable, keep others stable, and record outcomes.
Trap #4: Ignoring documentation
Minimal tracking can make a huge difference. I suggest noting: date, dose delivered (mcg), injection volume, injection site, and any immediate effects. This turns “I think it’s working” into something more testable.
Safety and quality considerations that directly affect dosing outcomes
Safety is not separate from dosing—it’s part of the dosing system.
Sterility and proper handling
Improper handling can increase contamination risk and also impact the reliability of your planned “dose vs. effect” relationship. Use appropriate sterile technique, clean work surfaces, and follow any handling instructions provided with your specific product.
Purity and concentration accuracy
Even with correct math, product quality matters. If you’re using a peptide that is not clearly specified (purity, concentration, or batch testing), your outcomes can be inconsistent. I strongly favor products with transparent specs and lot information.
Adverse effects monitoring
If you experience unexpected reactions (persistent irritation, rash, systemic symptoms), stop and seek appropriate medical guidance. For injection-based protocols, the “right” dosing plan includes a monitoring plan, not just a number.
Practical checklist for executing ghk cu dosing correctly
| Stage | What to verify | Why it matters |
|---|---|---|
| Before mixing | Vial peptide amount (mg/mcg) and any label instructions | Prevents wrong starting assumptions |
| Reconstitution | Exact diluent volume (mL) and method | Determines concentration and delivered dose |
| Syringe setup | Correct conversion between syringe markings and mL/µL | Avoids scale misreads |
| Injection | Measured injection volume (mL) and consistent technique | Maintains repeatable exposure |
| Tracking | Date, dose delivered, injection notes, any reactions | Enables interpretation and safer adjustment decisions |
FAQ
How do I calculate ghk cu dosing if my vial is labeled in mg?
Convert mg to mcg (1 mg = 1000 mcg), calculate concentration using (mcg ÷ mL reconstitution volume), then compute delivered dose as (concentration × injection volume). If you use syringe units, convert to mL/µL first based on your syringe’s scale.
What dosing schedule is best for GHK-Cu peptide injections?
There isn’t one universally “best” schedule—plans are typically chosen to balance tolerability, consistency, and the ability to interpret results. A common structure is starting conservatively, maintaining a stable frequency for a defined observation window, and changing only one variable at a time if adjustments are needed.
What should I do if I’m not noticing effects?
First, confirm your math and execution: reconstitution volume, concentration, syringe reading conversions, and injection volume. Then review consistency and tracking. If you still see no meaningful signal after a stable window, reassess the plan with appropriate professional guidance rather than increasing dose impulsively.
Conclusion
Good ghk cu dosing isn’t about finding a single number—it’s about delivering the correct dose with consistent concentration, correct syringe measurement, and a schedule you can actually evaluate. My best results from real-world protocol work have come from strict calculation checks, stable dosing windows, and simple documentation that turns “maybe it’s working” into something measurable.
Next step: Write down your vial amount, your reconstitution volume, and your planned injection volume, then calculate your dose per injection (mcg) and verify your syringe-unit conversion before you start.
Discussion