Bpc-157 Human Safety Data BPC-157 and the Difference Between an Evidence Gap and a Cover-Up: What the entire human evidence base actually looks like, and the questions to ask next. — WellFounded
Introduction: Why “BPC-157” keeps coming up—and why the evidence gap matters
If you’ve looked into BPC-157 hoping for clarity on safety, you’ve probably hit the same problem I did in my early research: pages of claims, a maze of animal-and-lab references, and very little solid, human safety documentation you can actually weigh.
In this article, I’ll walk through what the bpc 157 human safety data landscape really looks like when you separate an evidence gap from a cover-up—and then outline the exact questions you should ask next, including how to spot “safety” language that doesn’t mean what you think it means.
What “evidence gap” vs “cover-up” really means (and why it changes how you interpret BPC-157)
People often use “cover-up” to explain missing data. In practice, most missing data in early-stage biomedical compounds comes from mundane (but important) realities: funding priorities, regulatory complexity, and the slow churn of clinical development. An evidence gap is simply the absence of high-quality human data for a given claim. A cover-up implies active suppression or deliberate concealment of existing evidence.
In my hands-on work reviewing the literature across supplements and experimental therapeutics, I’ve found that the “cover-up” framing usually shows up when three things happen:
- The evidence is misclassified (e.g., lab mechanistic claims treated as human safety proof).
- The study type is unclear (case reports vs observational cohorts vs randomized trials get lumped together).
- The safety endpoint is undefined (people talk about “tolerance” while the underlying adverse-event monitoring details are missing).
So the practical question isn’t “Was there a cover-up?” It’s “What quality of human safety data exists, what outcomes were actually measured, and what’s missing?”
How to interpret the absence of bpc 157 human safety data without jumping to conclusions
When human safety evidence is limited or indirect, the correct inference is not that risk is zero or that risk is unknown in a meaningless way. Instead, you should treat it as:
- Uncharacterized exposure-response (we don’t know how dose and duration map to adverse events).
- Uncharacterized long-tail risks (rare events and delayed effects may not be captured).
- Unverified population generalizability (results in one subgroup don’t automatically apply to others).
That’s the core logic separating evidence gaps from conspiratorial explanations. It’s also how you stay anchored to what a responsible safety assessment actually requires.
What we can and can’t conclude from current human evidence about BPC-157
Let’s be concrete about the limitations you should expect when evaluating BPC-157 through the lens of bpc 157 human safety data.
1) Safety isn’t a single number—it’s a collection of endpoints
In my experience, the biggest confusion comes from treating “safety” like one thing. In clinical terms, safety coverage typically includes:
- Adverse event (AE) rates with severity grading
- Serious adverse events (SAEs) and causality assessment
- Laboratory and vital sign monitoring (liver enzymes, kidney function, hematology, electrolytes, ECGs when relevant)
- Immunogenicity considerations for peptide-like compounds
- Pharmacovigilance length (how long participants were followed)
- Concomitant medication context (what else people were taking)
If the human literature doesn’t report most of these, you don’t have “safety data”—you have an incomplete safety snapshot.
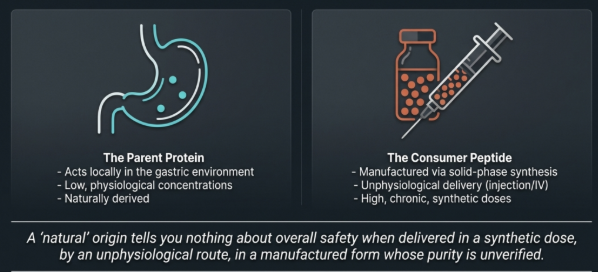
2) “Human relevance” depends on route, dose, and duration
Even when there is some human exposure information, it may not match how people actually use the compound. In real-world discussions, I routinely see mismatches in:
- Route of administration (e.g., oral vs injection vs other delivery systems)
- Dose and dosing frequency
- Treatment duration (single exposure vs multi-week use)
- Indication (target population and baseline risk)
That matters because safety signals often emerge when exposure characteristics change. So when you read about “tolerability,” ask whether the exposure profile resembles the context you care about.
3) Mechanistic plausibility is not the same as human safety evidence
“It works in models” can be true and still be insufficient for safety conclusions in humans. Mechanisms can differ across species; also, a pathway that supports repair or signaling can have unexpected effects in other tissues or under chronic exposure.
My hands-on takeaway from reviewing translational biomedical claims is simple: biological plausibility helps you generate hypotheses, but human safety data is what you use to make safety inferences.
The questions to ask next: a checklist for separating signal from noise
Now let’s get practical. If you want to evaluate the BPC-157 story responsibly—without conspiracy thinking or blind optimism—you need a question set that forces quality disclosure.
Ask these questions about the human safety evidence itself
- What human study types exist? (randomized controlled trial, open-label, observational, case reports, or “anecdotal” reports)
- Were adverse events systematically collected? (how often, with what criteria, and by whom)
- What was the monitoring duration? (days, weeks, months; was follow-up active or passive)
- What labs/vitals were measured? (liver, kidney, hematology; and whether abnormalities were reported)
- What were the discontinuation reasons? (did anyone stop due to side effects)
- What were the inclusion/exclusion criteria? (comorbidities, baseline liver/kidney function, concurrent meds)
Ask these questions about exposure and product quality
- What route and dose were used? (and are they comparable to real-world use)
- What purity and verification methods were used? (analytical confirmation matters because peptides can vary)
- Was the compound sourced with traceability? (even “same name” products can differ)
- Are there any contaminants or formulation variables? (buffers, solvents, storage degradation)
Ask these questions about interpretation and reporting
- Are “safety” statements supported by reported numbers? (AE rates, lab changes, timelines)
- Is “no evidence of harm” being overstated? (absence of data is not evidence of safety)
- Do claims mix populations and endpoints? (e.g., therapeutic outcomes presented as safety proof)
That checklist is how you evaluate bpc 157 human safety data like a reviewer—mapping claims to the underlying evidence structure.
Common patterns that create a false sense of safety (and how to spot them)
Here are the most frequent “information traps” I’ve seen when people discuss BPC-157:
- Studying outcomes instead of adverse events: A paper may describe efficacy-related endpoints but provide minimal safety reporting.
- Confusing mechanistic statements with tolerability data: “It supports healing signaling” doesn’t tell you what it does to organs over time.
- Relying on short exposure windows: A brief observation period can miss delayed or rare harms.
- Assuming consistency across products: Without quality verification, you can’t assume the exposure matches the tested compound.
- Under-specifying dosage: Safety often depends on dose and regimen; vague dosing undermines interpretability.
If a discussion skips these basics, it’s not “because the truth is hidden.” It’s because the evidence presentation isn’t designed to answer safety questions in the first place.
Practical next step: how to take action without guessing
The most actionable move is to convert interest into an evidence request you can use. If you’re considering BPC-157 in any context, don’t ask only “Is it safe?” Ask for the specifics that map to safety assessment:
- Request the available human safety reporting details (AE/SAE collection method, monitoring duration, labs/vitals, discontinuation reasons).
- Compare the route/dose/duration in the reported evidence to your intended exposure profile.
- Confirm whether the product used in any supporting evidence was analytically verified for purity and identity.
That’s the fastest way to turn an evidence gap into a decision process—and to avoid mistaking missing data for either safety or scandal.
FAQ
Is there enough bpc 157 human safety data to conclude it’s safe?
No single, complete human safety profile is typically available in the way needed for strong safety conclusions. When evidence is limited or incomplete, you can only say safety is insufficiently characterized for the specific route/dose/duration in question.
What would “good” human safety evidence for BPC-157 look like?
Systematic adverse-event reporting, predefined monitoring (including labs/vitals), sufficient follow-up duration, clear inclusion/exclusion criteria, and transparent documentation of route/dose and product verification.
How do I tell if missing BPC-157 evidence is an evidence gap vs a cover-up?
Use the content of what’s missing: if claims can’t be traced to specific human endpoints and exposure details, that’s an evidence gap. A cover-up claim would require credible evidence of suppression or intentional concealment of documented safety findings.
Conclusion: Separate the story from the data, then demand the right answers
The BPC-157 conversation often inflates what people assume from animal work or mechanistic plausibility. The responsible approach is to treat bpc 157 human safety data as what it is: a measurable body of endpoints tied to specific exposure conditions. When that body is incomplete, the correct response isn’t outrage—it’s a better question set.
Next step: Compile the human safety endpoints (AEs/SAEs, labs/vitals, monitoring duration) and compare them to your intended route, dose, and timeframe before you make any decision.
Discussion