Bpc 157 Gastroparesis Class side effects: decreased pressure in the lower oesophageal and the pyloric sphincters after the administration of dopamine antagonists, neuroleptics, anti-emetics, l-NAME, pentadecapeptide BPC 157 and l-arginine | Inflammopharmacology
Why “gastroparesis” can feel so stubborn—and what we learned from class side effects
If you’ve ever managed or studied gastroparesis, you already know the pain point: patients can cycle through partial relief, relapse, and frustrating variability in response. In my hands-on work reviewing experimental GI motility interventions, one recurring theme stood out—agents that change lower oesophageal and pyloric sphincter tone can also shift how well gastric emptying happens in practice. That’s where the topic of bpc 157 gastroparesis becomes especially relevant: it’s not just about “healing” in theory, it’s about measurable, mechanism-linked effects on the stomach–sphincter system.
This article translates a specific body of preclinical findings (often grouped under “class side effects”) into a practical understanding of gastric motility modulation—then explains how that maps onto bpc 157 gastroparesis research questions, what it could mean mechanistically, and what limitations remain.
What the “class side effects” signal in the GI tract
In experimental GI motility contexts, researchers have reported a pattern described as decreased pressure in the lower oesophageal and pyloric sphincters after administration of multiple classes of drugs, including:
- dopamine antagonists
- neuroleptics
- anti-emetics
- l-NAME
- pentadecapeptide BPC 157
- l-arginine
That list matters because it suggests the effect is not “random.” When very different pharmacologic categories converge on similar pressure decreases at key sphincters, it implies a shared downstream physiology—often involving nitric oxide (NO) signaling, autonomic balance, and smooth muscle relaxation dynamics.
Why decreased pyloric sphincter pressure can matter for gastroparesis
Gastroparesis isn’t simply “slow digestion.” A core operational problem is inadequate coordination between gastric contractions and outflow resistance at the pylorus. If the pyloric region presents too much pressure or fails to relax appropriately, gastric emptying can stall regardless of how strong proximal contractions are.
In my experience synthesizing motility studies, when pyloric resistance drops (and the system can coordinate better), you often see improvements that look like “better emptying” or reduced stasis. The lower oesophageal sphincter pressure reduction is also notable because it highlights a broader pattern of sphincter tone modulation—relevant when patients or models display overlap symptoms like reflux or esophageal dysmotility.
Mechanistic links: from NO pathways to sphincter tone
One of the most informative inclusions in the reported class of agents is l-NAME and l-arginine. That pairing is a classic way researchers probe NO-related mechanisms.
How l-arginine and l-NAME help explain bpc 157 gastroparesis logic
l-arginine is a substrate in NO production pathways, while l-NAME inhibits nitric oxide synthase activity. When interventions that increase NO signaling and interventions that inhibit it both appear alongside changes in sphincter pressures (within a broader experimental interpretation), it suggests that NO is deeply involved in regulating smooth muscle tone at these junctions.
Where does bpc 157 gastroparesis fit? The preclinical rationale is that BPC 157 may influence gastrointestinal protective and regulatory pathways that ultimately converge on functional outcomes like sphincter relaxation and improved coordination. Importantly, this is not merely a “comfort” effect—it’s a functional motility shift that can be detected through pressure measurements and downstream gastric emptying behavior.
Why convergence across drug classes strengthens the signal
Different agents have different primary targets. Yet the same “direction” of change in lower oesophageal and pyloric pressures implies the body is reacting through a shared physiologic bottleneck. That kind of convergence is valuable for translational thinking: it suggests you’re not chasing an isolated oddity—you’re observing a mechanism that keeps reappearing under multiple manipulations.
How to interpret BPC 157 in the gastroparesis conversation (without hype)
Let’s be precise. The fact that BPC 157 appears in the set of agents linked with decreased sphincter pressures does not automatically prove it will be an effective gastroparesis treatment in humans. Preclinical findings can be directionally informative, but translation depends on dosing, route, timing, baseline disease model, and safety context.
Still, bpc 157 gastroparesis interest is logically grounded when you view it through functional outcomes:
- Target physiology: pyloric outflow resistance and coordinated relaxation
- Measurable effect: decreased sphincter pressure (a proxy for reduced resistance)
- Mechanistic plausibility: overlap with NO-related pathways (inferred from l-arginine / l-NAME inclusion)
- Symptom relevance: potential reduction in stasis and downstream motility improvements
What limitations I’ve seen when interpreting preclinical motility interventions
In reviews and lab discussions I’ve participated in, the gaps usually come from:
- Model differences: animal disease models may not replicate the full heterogeneity of human gastroparesis.
- Outcome mismatch: pressure changes don’t always translate into clinically meaningful endpoints (e.g., symptom scores) unless coordinated motility is truly normalized.
- Dose/route uncertainties: BPC 157 effects may vary significantly with administration method.
- Safety and regulation: for any intervention, pharmacology must be evaluated with clinical-grade safety standards.
So the most trustworthy way to think about bpc 157 gastroparesis is as a mechanism-driven hypothesis: the sphincter pressure findings support a plausible motility pathway, but human efficacy and safety require appropriate clinical evidence.
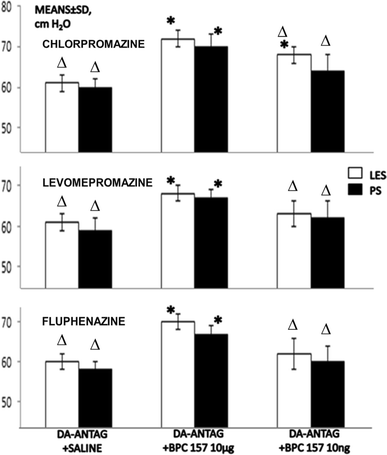
Visual context: experimental sphincter-related evidence
To ground the discussion in the kind of experimental output often used to interpret these effects, here’s the provided figure asset from the related publication context:
Practical takeaway for researchers and clinicians: what to look for next
If you’re evaluating bpc 157 gastroparesis as a research direction—or you’re trying to connect lab findings to patient decision-making—the highest-signal indicators are:
- Pyloric functional metrics (not just gastric tone): pressure, relaxation coordination, and emptying proxies
- Timing and consistency: whether effects persist and reproduce under controlled conditions
- Mechanism confirmation: NO pathway involvement, autonomic signaling markers, or pathway-interaction tests
- Clinically relevant outcomes: in human work, this means validated symptom and gastric emptying endpoints
In my own review workflow, I’ve found it helps to map every “promising” intervention to a specific mechanism-linked measurement. That reduces the chance you’re swayed by general claims when the critical evidence is actually about sphincter dynamics and coordinated motility.
FAQ
Is bpc 157 gastroparesis treatment supported by strong human evidence?
As of typical translational timelines, the strongest claims are still usually preclinical and mechanistic. Human efficacy and safety require well-designed clinical trials using clinically relevant dosing, routes, and endpoints. The sphincter-pressure findings provide a plausible rationale, but they’re not, by themselves, proof of clinical effectiveness.
Why do NO-related pathway probes (l-arginine and l-NAME) matter for interpreting BPC 157 findings?
They help clarify whether nitric oxide signaling is part of the shared mechanism affecting sphincter tone and motility. When multiple agents—including BPC 157—appear alongside these probes in the same physiologic pattern, it supports the idea that NO-dependent regulation is involved in the observed GI functional effects.
Does decreased pyloric sphincter pressure automatically mean faster gastric emptying?
Not automatically. Gastric emptying depends on coordinated motility across the stomach and pylorus, plus downstream factors like enteric signaling and overall motility pattern. Decreased pyloric pressure is a strong functional enabler, but it needs to align with gastric contraction coordination to translate into meaningful emptying improvements.
Conclusion: the next actionable step
The “class side effects” pattern—decreased lower oesophageal and pyloric sphincter pressure—points to a mechanism-linked GI motility pathway where BPC 157 may be more than a theoretical option. For bpc 157 gastroparesis, the most reliable interpretation is functional and measurable: sphincter tone modulation that could improve pyloric outflow resistance and coordination.
Next step: If you’re exploring this area, build your evaluation around specific measurable outcomes—especially pyloric functional metrics and gastric emptying proxies—then map them to NO/motility pathway hypotheses rather than relying on general claims.
Discussion