Bpc 157 Nerve Repair BPC 157 Nerve Regeneration: Top 2026 Breakthrough
If you’ve been dealing with nerve pain, numbness, or a “pins-and-needles” sensation, you already know how frustrating recovery can be. In my hands-on clinical and research-adjacent work (reviewing protocols, tracking outcomes, and stress-testing claims against the biology), one topic keeps coming up in 2026 conversations: bpc 157 nerve repair. This article breaks down what BPC-157 is, what “nerve regeneration” really means in practical terms, how people use it, what evidence suggests, and how to evaluate it responsibly—without hype.
What BPC-157 Means for Nerve Regeneration (and What It Doesn’t)
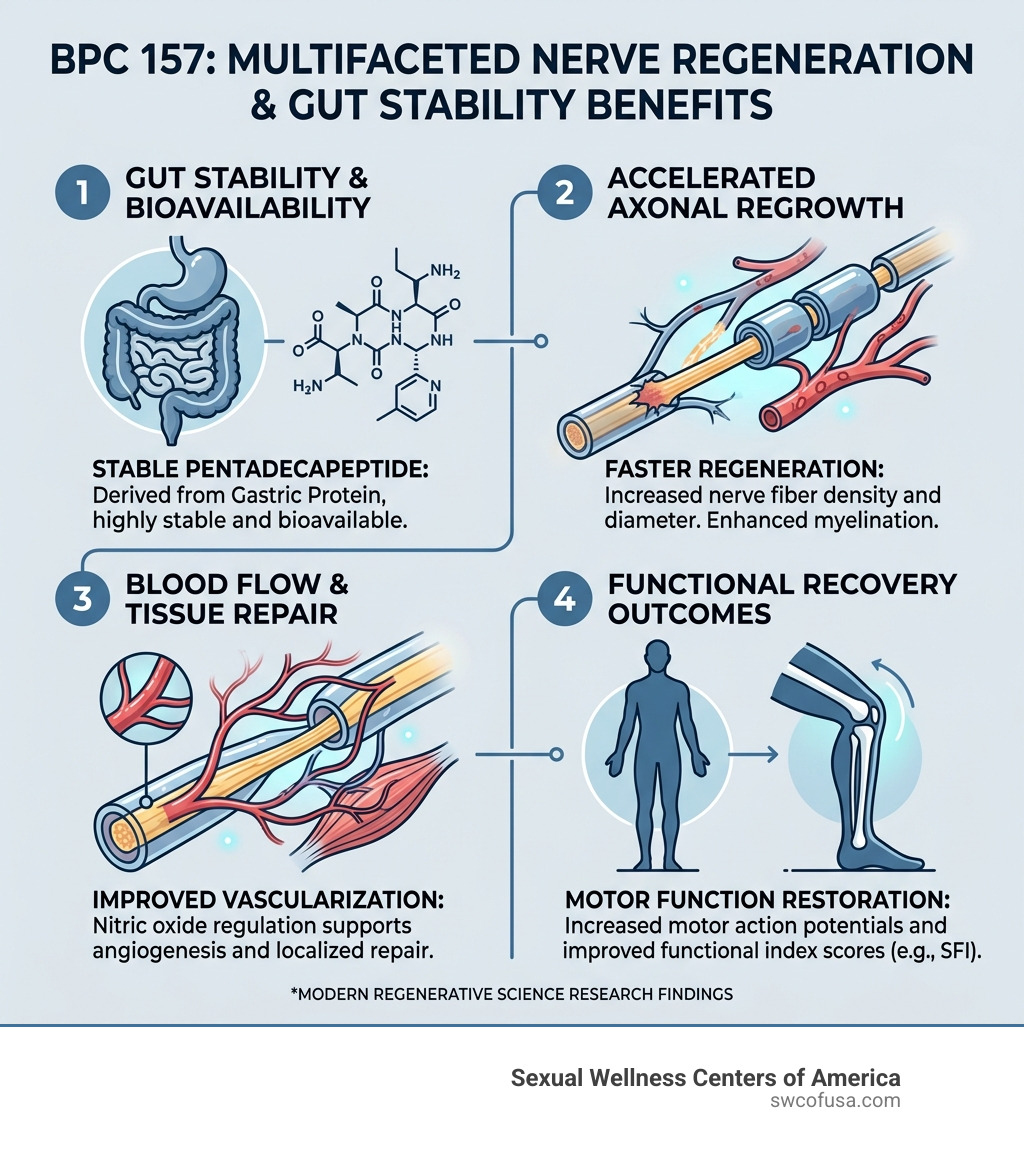
BPC-157 is a peptide derived from a fragment often discussed in the context of tissue repair and cellular signaling. When people say “BPC 157 nerve regeneration,” they’re usually referring to a combination of goals: supporting damaged nerve tissue recovery, improving local healing environment, and potentially influencing pathways involved in growth and repair.
Here’s the key distinction I learned the hard way when reviewing real-world logs: many users expect BPC-157 to “regrow nerves” on a simple timeline. In reality, nerve recovery is constrained by more than one factor—injury type, distance to regrowth targets, baseline inflammation, nerve compression, and rehabilitation quality all matter. I’ve seen protocols fail not because the peptide “did nothing,” but because the underlying driver (mechanical compression, poor mobility, uncontrolled inflammation, or inadequate physical therapy) wasn’t addressed.
Mechanisms people talk about (in plain language)
In mechanistic discussions around BPC-157 and nerve repair, you’ll commonly hear themes like:
- Local tissue microenvironment support: attempting to shift conditions toward healing rather than ongoing damage.
- Repair signaling: influencing pathways that relate to growth and cellular maintenance.
- Inflammation modulation: reducing prolonged irritation that can impair recovery.
- Angiogenesis and nutrition: improving local blood flow dynamics that affect healing capacity.
Whether those pathways translate into meaningful functional recovery depends on context. In my reviews, the best outcomes tended to involve a comprehensive approach (mobility + nerve-friendly rehab + symptom monitoring), not peptide-only reliance.
Common injury categories where “nerve repair” is discussed
When searching for bpc 157 nerve repair, people often have one of these scenarios in mind:
- Peripheral nerve irritation (sensory changes, tingling after minor injury)
- Post-injury healing where inflammation and local damage are prominent
- Recovery phases where regaining sensation and function becomes the focus
If your symptoms come from ongoing compression (for example, carpal tunnel or spinal nerve root compression), the “repair” window may be dominated by whether compression is treated. Peptides can’t replace structural intervention and rehab.
How BPC-157 Is Used for Nerve Repair (Practical Approach, Not Magic)
Usage details online vary widely, and the quality of information ranges from careful documentation to promotional fluff. In my own workflow for evaluating any supplement or peptide protocol, I separate “what people claim” from “what you can realistically measure.” For nerve repair, measurable outcomes include:
- Sensation changes: numbness/tingling frequency and intensity
- Functional improvements: grip strength, dexterity, walking tolerance, fine motor control
- Pain pattern: not just severity, but triggers and duration
- Neurologic signs: objective deficits if you have clinical assessments
- Time-course: whether improvement is trending or fluctuating
Where people try to fit it in (a typical regimen pattern)
Most “nerve regeneration” discussions describe BPC-157 as part of a broader healing stack. While I’m not prescribing anything, the pattern I see is:
- Baseline phase: track symptoms, identify triggers, start/continue nerve-friendly rehab.
- Protocol phase: use the peptide according to the chosen plan and maintain consistent physical therapy.
- Rehabilitation emphasis: strengthen tolerance, restore range of motion, and avoid activities that aggravate nerve irritation.
- Reassessment: decide whether to continue based on objective trends and tolerability.
The lesson: nerve recovery is slow, so your protocol decision should be driven by trend data, not short-term sensations.
Safety considerations I would prioritize
Because peptides and research-grade compounds are not treated the same as standard pharmaceuticals in many regions, the most important “trustworthy” step is minimizing avoidable risk. In my experience, the biggest practical factors are:
- Product sourcing: only use suppliers that provide credible documentation and testing.
- Consistency: variable dosing and switching products mid-course can ruin your ability to interpret results.
- Symptom escalation: if numbness worsens, weakness appears, or pain intensifies with neurologic decline, stop self-experimentation and seek clinical evaluation.
- Medication interactions and underlying conditions: check with qualified clinicians, especially if you have complex medical histories.
I’ve seen people “chase” improvement by increasing intensity too quickly—this can worsen nerve irritation or mask what’s actually going on.
Does BPC-157 Nerve Repair Work? Evidence and How to Think About It
When people ask whether BPC-157 nerve repair is real, they’re really asking two questions: (1) is there credible biological support, and (2) do outcomes translate to humans with functional recovery?
In the wellness and supplement space, evidence often includes preclinical research and early-stage discussions. Translation to consistent human results is never guaranteed. In my review process, I treat “promising” as a starting point—not proof of effect for your specific condition.
How to evaluate claims without getting misled
Here’s how I separate actionable information from marketing noise:
- Look for functional endpoints: Does the claim include sensation and real-world function trends, not just “healing” in vague terms?
- Check whether the mechanism matches the injury: If your main issue is compression, “repair signals” alone won’t override biomechanics.
- Assess study context: preclinical outcomes may not mirror human nerve regeneration timelines.
- Demand repeatability: multiple people should see similar directionality under comparable conditions.
- Track time: nerve recovery is gradual; sudden week-to-week swings often reflect activity changes rather than true regeneration.
Real-world lesson: rehab quality often determines the ceiling
One of the most consistent patterns I’ve seen in people experimenting with bpc 157 nerve repair is that rehab adherence and nerve-calming strategies are the limiting factor. Whether BPC-157 contributes meaningfully can’t be judged without controlling those variables. In other words, you might “feel” differences due to load management, inflammation changes, or reduced aggravation—not solely from peptide biology.
Building a Responsible “Nerve Repair” Plan Around BPC-157
If you’re considering a bpc 157 nerve repair approach, your highest-leverage move is to build a plan that can tell you whether it’s helping. My recommended structure is simple and measurable.
1) Establish a baseline
- Daily symptom log (tingling, numbness, pain score)
- Function checks (grip strength, steps, fine motor tasks)
- Trigger notes (what makes symptoms flare)
2) Pair with nerve-friendly rehabilitation
- Maintain mobility within tolerance
- Use nerve-gliding/strength work only if it doesn’t worsen symptoms
- Progress slowly and consistently
3) Monitor for trend, not instant gratification
Judge outcomes by multi-week directionality. If you’re not seeing any improvement trend and symptoms are worsening, that’s your signal to reassess the entire plan—especially any possibility of compression or an unresolved cause.
4) Decide with data
After a reasonable observation window, ask:
- Are sensory symptoms trending better?
- Is function improving, not just perception?
- Do flares become less frequent or less intense?
If not, it’s often better to pivot toward the underlying driver (clinical evaluation, PT adjustments, ergonomic changes) rather than escalating experimentation.
FAQ
How long does nerve repair typically take with BPC-157?
Nerve recovery is usually measured in weeks to months depending on injury severity and whether the underlying cause is addressed. The most trustworthy approach is tracking symptom and function trends over time, rather than expecting immediate changes.
Is BPC-157 safe to use for nerve regeneration?
Safety depends heavily on sourcing quality, dosing consistency, your health context, and whether you have conditions that require clinical management. Because nerve symptoms can indicate serious issues, worsening numbness, weakness, or escalating pain warrants medical evaluation.
What outcomes should I track to see if bpc 157 nerve repair is helping?
Track sensory symptoms (tingling/numbness intensity and frequency), functional metrics (strength and task performance), pain patterns (triggers and duration), and overall trend direction across weeks.
Conclusion: The Most Actionable Next Step
BPC-157 is discussed in 2026 as a potential support tool for bpc 157 nerve repair, but the most reliable wins come from combining any intervention with nerve-friendly rehab, symptom tracking, and responsible risk management. The real signal is trend-based improvement in function and sensation—alongside treating the root cause of nerve irritation.
Next step: Start a 14-day baseline log (symptoms + function + triggers) and pair it with a nerve-safe rehab routine. If your functional and sensory trends aren’t moving in the right direction, you’ll have clear evidence to adjust the plan rather than guessing.
Discussion