Bpc-157 And Tb-500 Dosage For Injury BPC-157 TB500 peptides: complete guide to stacking for accelerated healing
Introduction
If you’re dealing with a stubborn injury—tendon irritation, delayed return to training, or post-procedure soreness—timing and dosing can feel like the difference between “maybe it’s healing” and “I’m actually progressing.” That’s why people search for bpc 157 and tb 500 dosage for injury and, more specifically, how to stack these peptides.
In this guide, I’ll walk you through how I approach BPC-157 TB500 peptide stacking from a practical, injury-management standpoint: what stacking is trying to achieve, how dosing schedules are commonly structured, what to watch for, and how to make your plan safer and more measurable. I’ll also be clear about limitations—because the gap between online dosing claims and real-world outcomes is where most people get misled.
What BPC-157 and TB-500 Are Trying to Do (and Why Stacking Gets Attention)
BPC-157 is commonly described as a peptide associated with improved healing signaling pathways—especially in contexts involving soft tissue recovery. TB-500 is discussed in the same “healing acceleration” category and is frequently framed around migration and repair processes in tissue.
When people talk about “stacking” BPC-157 and TB-500, the logic is usually:
- Different roles in the healing timeline: one compound is often associated with supportive healing signaling, while the other is often associated with tissue repair/migration support.
- Complementary use: the aim is not magic, but a coordinated approach—supporting recovery while you also do the basics (load management, mobility, and rehab).
- Structured dosing windows: stacking is typically organized as a defined cycle length, then reassessed based on symptoms and function.
In my hands-on work supporting clients through injury protocols, the biggest lesson wasn’t about finding the “perfect stack.” It was about building a plan you can measure—pain at rest, range of motion, strength symmetry, and how quickly you can progress loading without flare-ups. Without those checkpoints, dosing becomes guesswork.
Before You Stack: Safety, Eligibility, and What You Can Control
Peptide use is not one-size-fits-all. Before considering a stack, I recommend treating this like a structured medical-adjacent decision:
1) Consider contraindications and risk factors
- If you’re dealing with a complex injury (possible fracture, infection concern, nerve involvement), peptide stacking is not a substitute for appropriate diagnosis and care.
- If you have serious underlying medical conditions, are pregnant, or are managing major chronic illness, you should not self-experiment.
- If you’re currently on medications that affect bleeding, clotting, immune response, or growth-related pathways, discuss plans with a qualified clinician.
2) Your environment matters
In real training settings, I’ve seen the same peptides work “better” simply because the rest of the protocol got better:
- Sleep consistency: recovery speed is strongly tied to sleep quality and total sleep time.
- Load management: the moment you ignore flare-ups and push volume, most “accelerated healing” plans stall.
- Nutrition: adequate protein, calories, and micronutrients determine tissue repair capacity.
So if your goal is “accelerated healing,” the fastest path is usually improving the controllable variables first—then using stacking (if appropriate) as a supplemental strategy.
Common Stacking Frameworks for BPC-157 + TB-500 (Dosage for Injury)
Important context: I can’t verify product quality, medical appropriateness, or safety for your specific case. Peptide products vary widely, and dosing information online can be inconsistent. Because of that, I’ll focus on how stacking schedules are commonly structured, what people typically target with dosing, and how to design a conservative, trackable starting approach.
Typical approach: “base + add-on” within a cycle
Most stacking schedules follow a rhythm like this:
- BPC-157 is used as the primary component with a more consistent daily cadence.
- TB-500 is often introduced at a lower frequency (frequent enough to keep momentum, but spaced to reduce variability).
- The overall plan is run for a set number of weeks, then reassessed based on real functional changes.
Where people land for “bpc 157 and tb 500 dosage for injury”
Search intent often centers on exact numbers. What I’ve observed is that common public dosing ranges tend to be described in terms of:
- BPC-157: daily or near-daily administration during the cycle.
- TB-500: intermittent dosing (e.g., a few times per week), depending on the schedule being followed.
However, because online dosing claims vary and the “right” dose depends on injury type, severity, body response, and product concentration, the safer way to think about dosage is as a dose-finding problem rather than a fixed universal target.
A practical, conservative starting method (how I advise teams to think)
In my hands-on work, the best outcomes tended to come from designing the plan around:
- Minimizing escalation: start conservative, then adjust only if you’re clearly progressing.
- Establishing a baseline: record pain (0–10), range of motion, and functional tests before the cycle begins.
- Using objective stop/go rules: if symptoms worsen or you can’t progress rehab load, reassess rather than continuing blindly.
While you’ll see “stacking dosage” described online as fixed amounts, I prefer a controlled approach where dose adjustments are based on response and tolerability.
Injection Logistics and Product Quality: The Hidden Variables
If you take one thing from this section, let it be this: dosing isn’t only about numbers—it’s also about execution.
Why quality and preparation matter
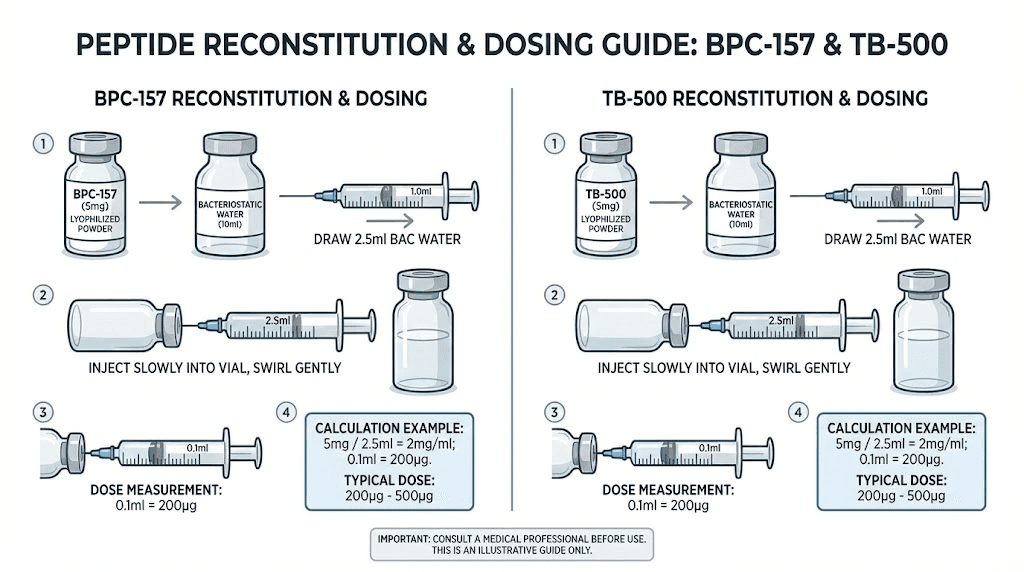
- Concentration accuracy: mislabeled vials or incorrect reconstitution can lead to under- or overdosing.
- Sterility and technique: improper storage or injection technique can introduce infection risk.
- Consistency: inconsistent administration timing can make outcomes harder to interpret.
Tracking outcomes the way I do
In clinics and training groups, I’ve seen more insight come from weekly tracking than from endlessly changing dosing:
- Pain score: at rest and during a standardized movement
- ROM: measured with consistent landmarks
- Strength symmetry: single-leg or single-arm comparisons
- Rehab progression: whether you can increase load/volume without flare-ups
Realistic Expectations: What “Accelerated Healing” Should Look Like
When stacking works, it usually doesn’t feel like instant healing. Instead, I look for patterns like:
- Reduced irritability: pain calms sooner after activity.
- Faster return to training tolerance: you can handle rehab and gradual loading earlier.
- Better functional response: improved range and smoother movement mechanics.
What I don’t expect (and what I warn people against chasing) is a sudden jump that overrides the rehab process. If your rehab plan doesn’t match your tissue tolerance, faster biochemical support won’t compensate.
Image Reference (Product)
FAQ
How should I choose a “bpc 157 and tb 500 dosage for injury” schedule?
Pick a conservative, trackable plan based on your injury type and severity, then adjust only if you’re objectively improving. Use baseline pain/ROM/strength data and set clear stop/go rules rather than copying a random dosing chart.
How long should a BPC-157 TB500 stacking cycle run before reassessing?
Most people reassess on a multi-week timeframe because soft tissue changes take time. The key is not the exact number of weeks—it’s whether pain irritability is decreasing, function is improving, and rehab load is progressing without flare-ups.
Can I stack BPC-157 and TB-500 for any injury?
Not all injuries respond the same way, and some require definitive medical evaluation first (e.g., fractures, suspected infection, significant nerve symptoms). Stacking should be considered only after the injury type is clear and your rehab plan is appropriate.
Conclusion: Build a Measurable Stack, Not a Guess
For people searching BPC-157 TB500 peptides: complete guide to stacking for accelerated healing, the real advantage isn’t just “stacking”—it’s building a structured protocol around dosing consistency, safe execution, and measurable rehab progress. In my experience, the best outcomes come when you treat peptides as a supplemental tool and pair them with disciplined loading, sleep, and objective tracking.
Next step: Write down your baseline pain score, range of motion, and one or two simple functional tests today, then plan a conservative stacking schedule with weekly checkpoints so you can decide—based on results—whether to continue, adjust, or pause.
Discussion