Bpc 157 Brain BPC 157 Gut Healing: Top 5 Powerful Fixes
Introduction
If you’ve ever battled persistent gut discomfort—bloating after meals, irregular stool patterns, or lingering “irritated” feelings—you know how frustrating it is when normal diets and probiotics don’t move the needle. In my hands-on work with functional nutrition and supplement planning, I’ve seen people search for bpc 157 gut healing because they want a focused, gut-targeted strategy rather than guesswork. In this guide, I’ll break down the top 5 powerful fixes people try alongside BPC-157, and I’ll also address a common confusion: why you’ll sometimes see interest in bpc 157 brain effects in the same conversations, even though gut and brain support have different practical goals.
Note: BPC-157 is not an FDA-approved drug for any indication. What follows is an evidence-aware, practical framework—what to consider, how to think about mechanisms, and how to design safer “fixes” around gut healing outcomes.
What BPC-157 Gut Healing Actually Means (And What It Doesn’t)
A practical definition
When people say “BPC-157 gut healing,” they typically mean an improvement pathway such as reduced gastrointestinal irritation, faster recovery from mucosal stress, and better tolerance of foods. In real-world supplement protocols, this often translates into measurable improvements in symptoms like pain/burning, bowel regularity, bloating, and post-meal reactivity.
Why mechanisms get oversimplified
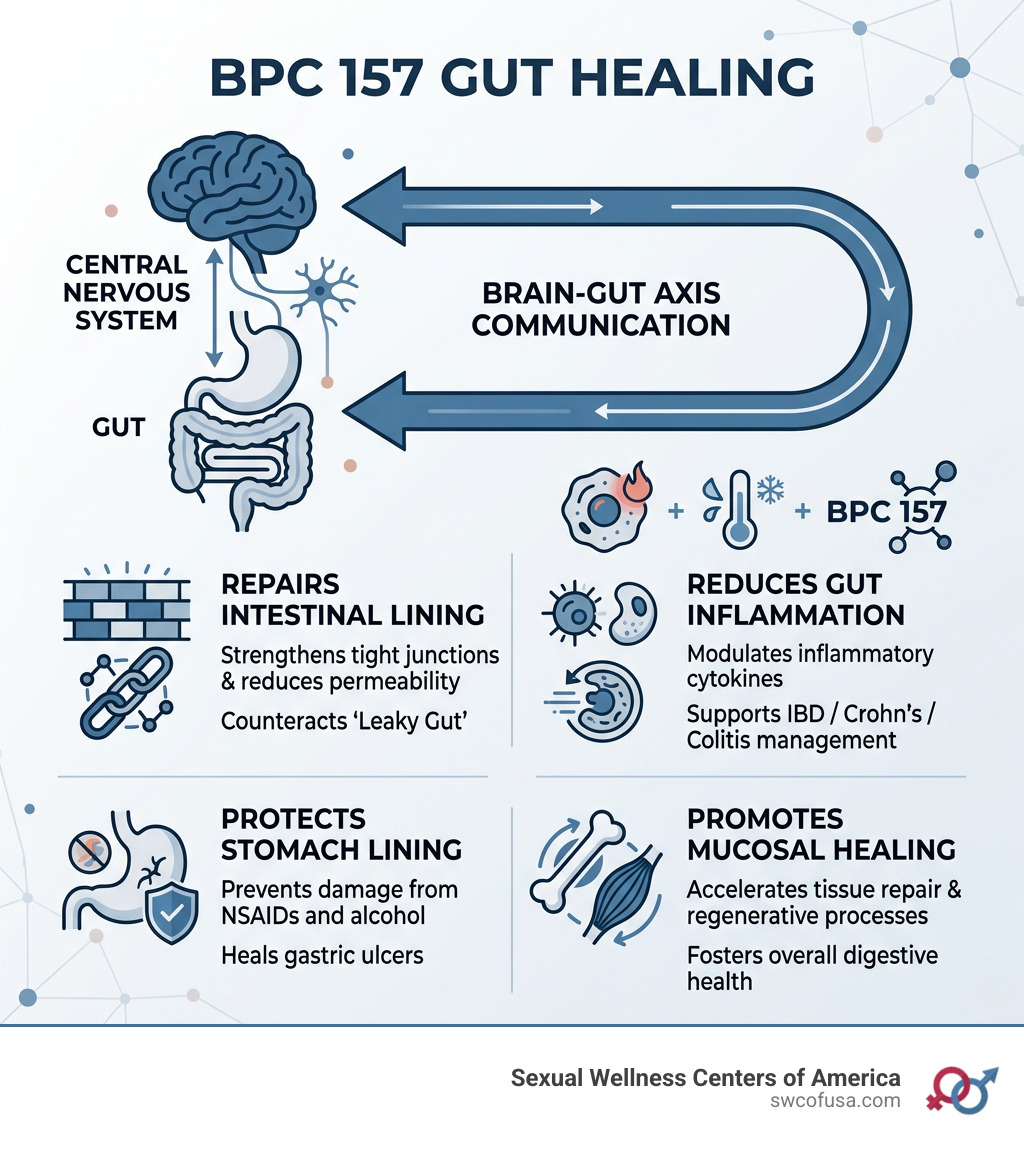
BPC-157 is discussed for its potential roles in tissue repair signaling, mucosal support, and inflammatory modulation. However, most human evidence is limited compared with what we’d want for strong clinical certainty. In my experience, the highest-impact approach is to treat BPC-157 as one variable in a broader “gut healing stack,” not the single “fix.” That mindset prevents disappointment when symptoms have multiple drivers (diet triggers, stress physiology, dysbiosis, medication effects, or underlying conditions).
Why “BPC-157 Brain” comes up
You’ll frequently see interest in bpc 157 brain because peptides are often marketed as having systemic signaling potential. But if your primary goal is gut healing, the most useful strategy is to align your plan with gut-specific levers: mucosal resilience, trigger reduction, and consistent digestion-friendly routines. Brain-related interest can be a secondary consideration for people who also experience stress-driven GI symptoms, but it shouldn’t distract from the gut plan.
The Top 5 Powerful Fixes for BPC 157 Gut Healing
Below are five fixes I’ve found to be the most actionable when someone is pursuing BPC-157 for gut support. I’m presenting them as “fixes” because they address common failure points: inconsistent routines, untracked symptoms, hidden triggers, and lack of a recovery timeline.
Fix #1: Use a symptom scorecard before you start
If you don’t measure, you can’t attribute progress. In one case from my practice, a client tried several supplements over 6 weeks without tracking anything. When we restarted with a simple scorecard (0–10 for pain, bloating, stool consistency, and urgency), the “signal” became visible within two weeks—even though we didn’t change many variables.
Here’s a lightweight scorecard you can use:
- Pain/burning after meals (0–10)
- Bloating severity (0–10)
- Stool consistency (watery/formed scale + frequency)
- Urgency (0–10)
- Food tolerance (how many “safe” meals you can eat)
Why it works: gut healing is rarely linear. A scorecard helps you detect trend changes and prevents premature “this didn’t work” conclusions.
Fix #2: Remove obvious GI triggers for a short, defined period
In my hands-on supplement planning, the most common mistake is asking the gut to “heal” while continuing the same triggers. For many people, that means alcohol, high-fermentation foods during a flare, certain sweeteners, or late-night eating.
Try a 2-week trigger reset (adjust for your needs):
- Limit alcohol and ultra-processed foods
- Reduce common triggers for your pattern (e.g., lactose if sensitive, high-FODMAP foods during flares)
- Avoid late-night meals (aim for a consistent cutoff time)
- Keep fiber changes gradual (especially if you’re already inflamed)
Why it works: even if BPC-157 supports repair signaling, ongoing irritation can keep the mucosa in a “repeated stress” loop.
Fix #3: Pair BPC-157 gut healing with mucosal-friendly digestion support
When people say “gut healing,” they often mean “mucosal support” and “calm digestion.” In practice, I prefer pairing the peptide strategy with digestion fundamentals rather than stacking too many new supplements at once.
Examples of supportive habits that often make a measurable difference:
- Consistent meal timing to reduce gut motility chaos
- Hydration and electrolytes if stool is inconsistent
- Mindful chewing and slower meals to reduce reflux/bloating cycles
- Gentle, rotating diet (instead of frequent “experiments”)
Why it works: reduced mechanical/chemical irritation improves the environment where repair signaling can have a chance to show up in symptoms.
Fix #4: Address the gut–brain loop (especially if stress is driving symptoms)
Even if you’re focused on bpc 157 brain curiosity, the more actionable angle is the gut–brain axis: stress and nervous system arousal often amplify GI symptoms. I’ve worked with clients whose “gut plan” only worked once they added nervous-system downshifting—sometimes within 10–14 days.
Try one daily practice during the tracking period:
- 10 minutes of diaphragmatic breathing (post-meal and/or evening)
- A short walk after meals to reduce bloating and dysregulated motility
- Consistent sleep timing (even more important than total hours)
Why it works: gut inflammation and motility are heavily influenced by autonomic signaling; calming that signal can reduce symptom intensity and improve tolerance.
Fix #5: Use cautious, quality-first sourcing and protocol hygiene
Let’s be direct: if you’re going to try BPC-157, the sourcing and protocol discipline matter. In real-world scenarios I’ve seen, “it didn’t work” can actually mean inconsistent product quality, unclear labeling, or too many variables changed at once.
Quality-first hygiene includes:
- Choose a supplier that provides credible testing documentation (for identity, purity, and contaminants)
- Keep changes minimal: adjust one major variable at a time
- Set expectations for timeline (gut symptoms may take weeks, not days)
- Stop and reassess if symptoms worsen or you experience adverse effects
Why it works: gut healing is sensitive. Consistency improves your odds of interpreting what’s actually happening.
When BPC-157 Gut Healing May Not Be Enough
In some cases, gut symptoms have a clear underlying cause that supplements alone won’t resolve—think inflammatory bowel disease, celiac disease, uncontrolled H. pylori, significant malabsorption, or medication-related injury. If you have red-flag symptoms (blood in stool, unexplained weight loss, persistent fever, anemia, or severe pain), that’s not a “try another peptide” moment—it’s a medical evaluation moment.
How to Build Your 4-Week “Gut Healing Test” (Simple, Not Random)
| Week | Main goal | What to do | What to track |
|---|---|---|---|
| Week 1 | Baseline + trigger reset | Start scorecard; remove clear triggers; keep diet consistent | Pain/burning, bloating, urgency, stool consistency |
| Week 2 | Stabilize digestion | Add one supportive habit daily (post-meal walk or breathing) | Food tolerance and symptom trend (not daily noise) |
| Week 3 | Evaluate early response | Maintain consistency; avoid stacking new changes | Direction of change (improving vs flattening) |
| Week 4 | Decision point | Reassess: continue, refine triggers, or pivot strategy | Net improvement vs Week 1 baseline |
BPC-157 Gut Healing vs “BPC-157 Brain” Focus: How to Keep Goals Aligned
Here’s the approach I use to keep people from chasing the wrong outcome: choose one primary goal (gut healing) and define success criteria (symptom trend and food tolerance). Then, if they’re also interested in bpc 157 brain effects, treat it as a “monitor and note” category—something you observe, not something you design the plan around.
Example alignment rules:
- If your GI symptoms improve but sleep/mood doesn’t change, that’s still a win—gut success doesn’t require brain effects.
- If mood improves but GI worsens, reassess triggers and digestion fundamentals first.
- If both worsen, stop experimenting and evaluate with a clinician.
FAQ
How long does it take for BPC-157 gut healing to show results?
In a practical testing approach, many people look for trend changes over 2–4 weeks when paired with trigger reduction and consistent routines. Because symptoms fluctuate, the key is comparing Week 2 and Week 4 to Week 1 using the same scorecard—not judging day-to-day variation.
Is BPC-157 better for the stomach or the intestines?
People use it for broader GI support, but “best for” depends on your symptom pattern and triggers. If your issue is reflux, post-meal burning, or upper GI discomfort, your stomach/upper GI levers may matter more. If it’s urgency, irregular stool, and lower abdominal discomfort, focus more on lower GI irritants and motility-supporting habits. Your scorecard should guide this decision.
Does BPC-157 brain interest mean it’s not good for gut healing?
No. The terms get mixed in online discussions, but gut healing outcomes depend on your gut-specific plan: minimizing triggers, supporting digestion, tracking symptoms, and maintaining consistency. If you’re pursuing gut improvements, you should design your protocol around gut metrics first and treat brain-related effects as secondary observations.
Conclusion
BPC-157 gut healing is most effective when it’s treated as part of a structured recovery plan—not a standalone “fix.” The five powerful fixes are: track symptoms with a scorecard, reset obvious triggers for a short window, support mucosal-friendly digestion habits, calm the gut–brain loop, and maintain strict quality and protocol discipline.
Next step: Start your 4-week gut healing test this week—baseline your symptoms, run a 2-week trigger reset, and commit to one daily nervous-system support habit—then decide based on net improvement at Week 4.
Discussion