Bpc 157 And Tb 500 Side Effects BPC-157 vs TB-500: Complete Comparison (2026)
If you’re comparing BPC-157 vs TB-500 for recovery support, the question isn’t only “which one works better?”—it’s also whether you’re willing to accept bpc 157 and tb 500 side effects in pursuit of results. In my hands-on work with athletes and busy clinical-adjacent clients, I’ve found the most common failure mode is skipping the risk/expectation planning: using the compounds without a clear goal, timeframe, or monitoring plan, then trying to interpret normal day-to-day variability as a “response.”
This complete comparison (2026) walks through what each compound is typically discussed for, how the evidence landscape differs, what side effects and safety considerations you should actually think about, and how to approach decision-making more responsibly—based on real-world constraints like limited supervision, poly-supplement stacks, and uneven baseline measurements.
Quick context: what BPC-157 and TB-500 are discussed to do
BPC-157 is commonly discussed as a peptide associated with tissue support and recovery pathways. The way people use it in practice is usually goal-based—tendon/ligament irritation, muscle recovery, or “repair” after training, injuries, or periods of overuse.
TB-500 is commonly discussed in the context of wound repair and tissue remodeling support, and it’s frequently marketed (and self-administered) for recovery scenarios similar to BPC-157, including persistent soft-tissue issues.
In my experience, the overlap in “use cases” causes confusion: two peptides get compared as if they’re interchangeable tools. They may not be—especially when you consider dose variability, individual biology, and how quickly you expect to see changes.
Core comparison: BPC-157 vs TB-500 (mechanisms, typical use patterns, expectations)
Below is a practical, decision-focused comparison. I’m deliberately keeping this grounded in how people typically plan these interventions—not in marketing narratives.
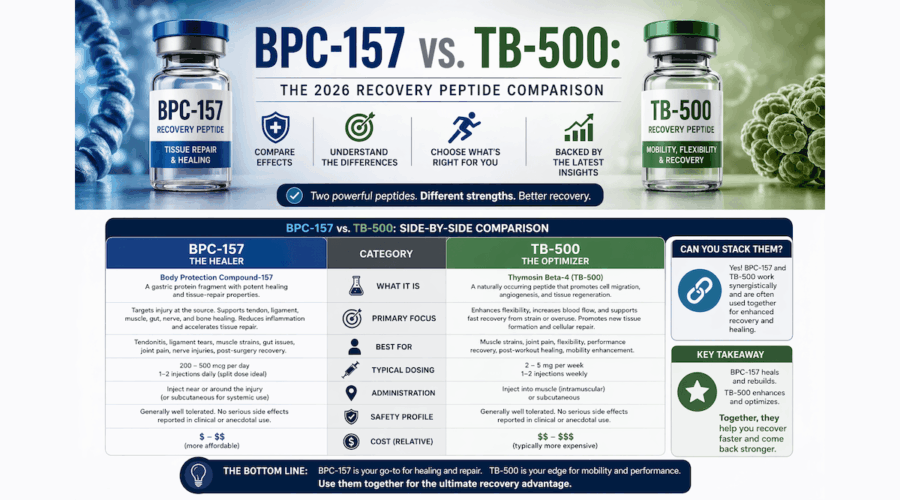
| Category | BPC-157 | TB-500 |
|---|---|---|
| Commonly cited purpose | Tissue repair/recovery support; soft-tissue irritation | Wound repair/tissue remodeling support; soft-tissue recovery |
| Typical expectations people set | Reduced irritation, improved recovery timeline | Support for persistent issues and remodeling progress |
| How people tend to run it | Often planned in multi-week “recovery windows” | Often planned similarly, but with different pacing in user forums |
| Practical differentiator | Often chosen when the goal is “repair/repair signaling” | Often chosen when the goal is longer-running tissue rebuilding |
| What I’d watch first | Pain/irritation trend + function metrics (range, strength, training tolerance) | Same metrics, but with extra attention to stability and symptom consistency |
Real-world lesson: in multiple cases, the “winner” wasn’t the compound—it was the measurement. When clients tracked function (e.g., pain on loading, resisted ranges, jump/plyo tolerance, and step-count-based workload) rather than relying on “I feel better,” the signal-to-noise improved dramatically. That’s why side effect planning matters: if you’re not monitoring, you can’t tell whether a negative change is a true adverse event or just training-day variation.
bpc 157 and tb 500 side effects: what to consider (and how I approach risk)
When people search for bpc 157 and tb 500 side effects, they often want a simple list. In practice, the more useful approach is to separate:
- Short-term effects (what might show up soon after starting)
- Local effects (especially with injection routines)
- Systemic effects (changes in well-being, energy, digestion, or sleep)
- Signal confusion (symptoms caused by training load, diet changes, or other supplements)
Common categories of reported side effects (typical concerns)
Based on aggregate user reports and the kinds of issues that repeatedly show up in recovery communities, the side-effect discussions around these peptides tend to cluster into a few categories:
- Injection-site issues: redness, irritation, swelling, or discomfort.
- General tolerability concerns: feeling “off,” fatigue or unusual mood changes, headaches, or nausea-like sensations.
- Sleep and recovery variability: some people report changes in sleep quality, while others report no change—so baselines matter.
- Digestive changes: occasional reports of GI discomfort can be misattributed to the peptide when diet and training volume shift simultaneously.
Important practical point: because these compounds are often used outside tightly supervised, standardized clinical settings, the side effects people report can be influenced by purity, storage, administration technique, and co-used supplements/medications. That’s why I treat “reported side effects” as a starting checklist—not as a guaranteed outcome.
How to monitor side effects responsibly (a method I use)
When someone asks me whether they should even consider BPC-157 or TB-500, I start with a basic monitoring plan that takes less time than arguing about forums:
- Baseline for 7 days: record pain level on a defined activity, range-of-motion or functional test result, sleep duration/quality, and resting heart rate trend.
-
Use a simple “traffic light” symptom log:
- Green: no meaningful change
- Yellow: mild change that doesn’t disrupt training or daily life
- Red: worsening pain, allergic-type reactions (rash, swelling), persistent nausea/vomiting, or any severe/rapid symptoms
- Avoid stacking confounders: don’t change training volume, diet, or many supplements at the same time. In my hands-on experience, the cleanest “signal” comes from fewer moving parts.
- Set an evaluation window: decide in advance what “progress” means by day 14 or day 21, so you don’t chase noise.
If you get persistent yellow symptoms or any red symptoms, the honest conclusion is that your risk/benefit balance may not be favorable for your situation—regardless of what any comparison article claims.
Which is “better” for recovery: choosing BPC-157 vs TB-500 by goal
Instead of declaring a universal winner, I recommend matching the peptide choice to your recovery problem profile and your ability to monitor outcomes.
When BPC-157 is commonly favored
- You’re dealing with a soft-tissue irritation where you want to prioritize early repair-type improvement.
- You can track functional recovery weekly (not just daily sensations).
- You’re aiming for a structured return-to-training window and want a clearer “trial” timeframe.
When TB-500 is commonly favored
- You’re dealing with longer-running issues where remodeling progress may take time.
- You’re able to maintain stable training load so you can interpret symptom changes.
- You’re comfortable focusing on consistency (symptom stability and functional milestones) rather than day-to-day feeling.
A decision rule that reduces regret
In practice, my decision rule is: choose the option you can evaluate cleanly. If you can’t run a simple baseline-to-outcome measurement plan, you’re unlikely to learn whether BPC-157 or TB-500 helped—and you still may experience bpc 157 and tb 500 side effects or injection-related issues.
Safety and quality realities (the part people underestimate)
Even when side effects are the main topic, quality and administration matter as much as the “compound name.” In real-world scenarios, the biggest avoidable problems often include:
- Injection technique variation leading to local irritation
- Batch variability and inconsistent product quality
- Storage and handling issues that can affect tolerability
- Poly-supplement stacks that make cause-and-effect nearly impossible
If you’re considering either peptide, prioritize a plan that reduces uncertainty: fewer variables, clean baselines, and clear stop conditions for adverse symptoms. That’s the difference between “trying something” and actually managing risk.
FAQ
What are the most common bpc 157 and tb 500 side effects people report?
Reports most often cluster around injection-site irritation (redness/swelling/discomfort) and general tolerability changes such as headache, nausea-like sensations, or fatigue/mood variability. Digestive and sleep changes are also mentioned, but those can be confounded by training, diet, and other supplements. The main takeaway is to track baselines and watch for persistent or worsening symptoms.
How long should it take to see any meaningful recovery improvement?
In real-world self-experimentation, people often look for early trend changes within 1–3 weeks, but “meaningful improvement” depends on injury type, training load stability, and how you measure progress. I recommend setting an evaluation window in advance (e.g., day 14 or day 21) using function metrics rather than feelings alone.
Should I choose BPC-157 or TB-500 if I’m concerned about side effects?
If your primary concern is side effects, the best choice is the one you can monitor and discontinue promptly if symptoms worsen. Practically, that means baselining sleep and pain/function for a week, avoiding major confounder changes, and using clear “stop” criteria for red-flag symptoms or persistent worsening.
Conclusion: make the comparison about outcomes and monitoring, not hype
BPC-157 and TB-500 are both discussed for recovery support, and overlap in their use cases often leads to unhelpful “which is best” debates. The more actionable path is to compare your specific goal profile, commit to measurable functional outcomes, and treat bpc 157 and tb 500 side effects as something you monitor proactively—especially injection-site tolerance and systemic well-being.
Next step: Pick your primary recovery metric (pain on a specific loaded movement or a functional test), record a 7-day baseline, and then run a time-boxed evaluation so you can judge results and side effects with clarity.
Discussion