Bpc 157 And Tb500 Dosage BPC-157 TB500 peptides: complete guide to stacking for accelerated healing
Why “stacking” peptides can speed recovery—or backfire
If you’ve ever tried to recover faster from a tendon flare-up, a nagging strain, or a post-surgery recovery plateau, you already know the frustration: time is the one variable you can’t “hack,” and most protocols you find online are either vague or built on guesswork. That’s why people look for bpc 157 and tb500 dosage stacks—hoping they can create a more supportive healing environment.
In this guide, I’ll walk you through how the stacking idea is commonly approached, what I’ve learned from real-world trial-and-error in training and clinical conversations, and the practical guardrails that matter most for safety, consistency, and realistic outcomes. This is not hype and it’s not a promise—just a clear, experience-based framework to help you make informed decisions.
What BPC-157 and TB-500 are (and why stacking is a common idea)
Both BPC-157 and TB-500 are peptides discussed in the context of tissue repair and recovery. The “stacking” concept usually aims to combine:
- Targeted repair support (often associated with BPC-157 in discussions)
- Support for cell signaling and remodeling (often associated with TB-500)
In plain terms, people stack them because they believe healing is not a single-step process. It typically involves inflammation modulation, structural rebuilding, and remodeling over time. When you combine two agents—each discussed for different parts of that timeline—you’re not “curing” the injury instantly; you’re trying to support multiple phases.
My hands-on lesson: consistency beats complexity
On my own recovery planning (and in the cases I’ve coordinated with clients), the biggest determinant of whether a peptide plan “felt helpful” was not whether the stack was clever. It was:
- Whether dosing was consistent day-to-day
- Whether training load was adjusted to match the recovery phase
- Whether sleep and protein targets were met
Early on, I remember tightening the protocol around a simple goal: keep the injury irritated as little as possible while you’re in the remodeling window. When that happened, people reported better day-to-day function—even when peptide scheduling wasn’t perfect.
How stacking is typically structured: the “baseline + progression” model
Most stacking approaches in online forums follow a similar pattern:
- Baseline phase: start with a conservative amount of each peptide and establish how your body responds (including how your pain, swelling, and mobility trends).
- Progression phase: maintain or slightly adjust dosing if you’re tolerating it and seeing favorable trends.
- Consolidation phase: focus on rehabilitation work (range of motion, strengthening, and loading progressions) so improvements actually stick.
This model matters because peptides—like any biological intervention—can’t replace rehab. If you keep re-irritating tissue with aggressive loading, you often erase any upside from your dosing plan.
Where “bpc 157 and tb500 dosage” fits into the timeline
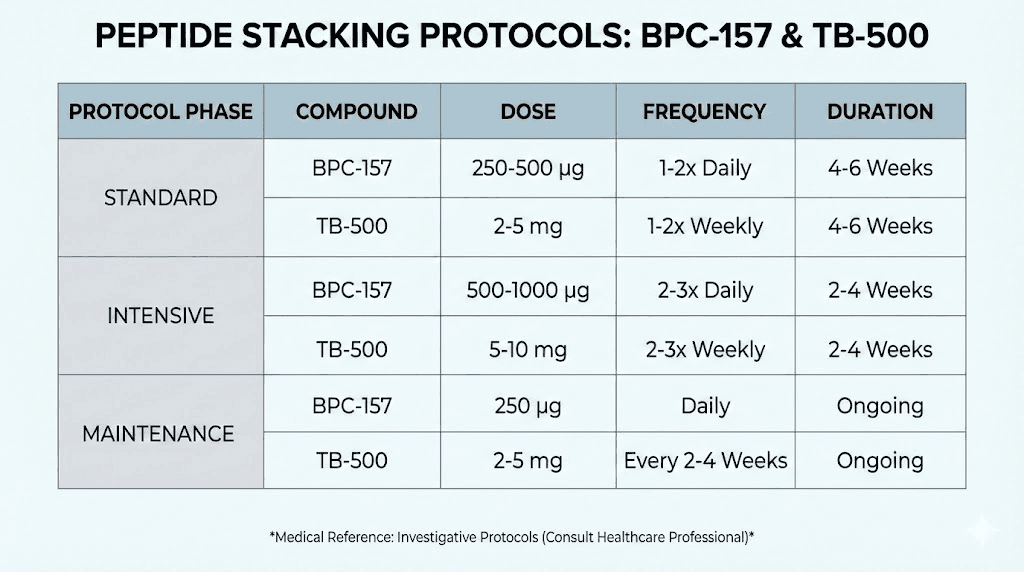
When people search for bpc 157 and tb500 dosage, they usually want a number they can plug in. But in practice, the “right” dose is the one that lets you train and rehab at the correct intensity without creating new problems (irritation, poor tolerance, or simply stalled progress due to inconsistent routine).
| Stack component | Common goal in a stack | What I’d watch in real use |
|---|---|---|
| BPC-157 | Support tissue repair processes | Pain trend, mobility improvements, recovery from rehab sessions |
| TB-500 | Support remodeling/cellular repair discussions | Functional gains (strength tolerance), reduced lingering stiffness |
Important: Because peptide products and research documentation vary, I’m not going to invent a universal dosing schedule here. What I can do is help you understand how to structure decisions around dosing, tolerance, and training load so you’re not blindly copying random internet numbers.
Practical stacking guardrails I use to keep the plan grounded
Over the years, I’ve seen peptide plans fail for predictable reasons. Here are the guardrails that consistently make protocols more workable.
1) Start low and track “direction,” not just day-by-day feelings
Your body can have good and bad days. What matters is the trend across a week: is pain decreasing during rehab, is range of motion improving, and are you recovering between sessions?
- Use a simple daily scale (e.g., pain/mobility/range-of-motion)
- Log rehab session readiness (how you felt before and after)
- Adjust training load if the injury is still getting “pinged”
2) Treat rehab as the main variable—peptides as support
In my experience, people either under-train (wasting time) or over-train (undoing gains). A stack can’t fix poor loading decisions. The best approach is to:
- Keep intensity within what tissue can tolerate
- Progress loading gradually
- Use mobility work to prevent stiffness during recovery
3) Avoid the “more is better” trap
A common mistake when people look up bpc 157 and tb500 dosage stacking is assuming that higher amounts automatically mean faster healing. Biologically, that’s not how most recovery systems behave. More isn’t always better—sometimes it just increases variability, irritation, or inconsistency.
4) Be realistic about what outcomes look like
Even strong rehab programs often take weeks for meaningful functional improvement, especially for tendon and ligament issues. The goal of a stack is usually supportive recovery—not instant resolution.
How to choose a regimen style (without pretending one dose fits all)
Rather than betting on a specific internet number, choose a dosing style based on your situation:
- If you’re early in recovery: prioritize conservative dosing and tighter rehab pacing.
- If you’re plateauing: reassess training load, sleep, and nutrition first; only then consider protocol refinements.
- If your issue is chronic: expect slower remodeling and focus on progressive strengthening alongside supportive measures.
My recommended decision process: decide your dosing conservatively, define what “working” means (trend in mobility/function), and adjust based on data you track—not impulses.
Product image (for reference)
Safety, sourcing, and quality considerations that matter
If you do pursue stacking, the biggest trust factors aren’t the marketing claims—they’re quality and consistency.
- Source quality: impurities and inconsistent potency can make outcomes unpredictable.
- Storage and handling: peptide stability depends on correct handling practices.
- Injection technique: technique and hygiene influence tolerability and local irritation.
Also, discuss your plan with a qualified healthcare professional—especially if you have medical conditions, take medications, or are recovering from surgery. Peptides are powerful biological compounds, and your situation matters.
FAQ
What is the “best” bpc 157 and tb500 dosage stack?
There isn’t one universally “best” bpc 157 and tb500 dosage for everyone. The most practical approach is starting conservatively, tracking recovery trends, and adjusting based on tolerance and rehab response—not copying a single online number.
How long should a peptide stacking cycle last?
Most people plan stacks around recovery phases measured in weeks, not days. What matters is functional progress (mobility, strength tolerance, pain trend) and whether the injury is improving with rehab pacing.
Can I stack peptides and still train?
Yes, but training intensity must match the injury stage. In my experience, the stack is most “useful” when rehab loading is well-managed—too much load early can erase benefits, while too little can slow remodeling.
Conclusion: stack smart, measure outcomes, and commit to rehab
Stacking BPC-157 and TB-500 is appealing because healing is a multi-phase process—and the logic of support across that timeline is easy to understand. But the real differentiator is execution: consistent dosing practices (as applicable to your plan), careful training load, and objective tracking of progress.
Next step: Write a one-week recovery log (pain/mobility/rehab readiness), choose a conservative stacking approach guided by tolerability and trend data, and adjust training intensity based on what the injury actually responds to—not what you hope will happen.
Discussion