Bpc 157 And Bone Healing Bpc 157 bone healing: 2025's Crucial Warning
Introduction: A “bone healing” claim you shouldn’t take at face value
If you’ve ever searched bpc 157 and bone healing because you’re dealing with a fracture, slow union, or persistent bone pain, you’ve probably seen bold claims and confusing dosing stories. In practice, the hardest part isn’t finding information—it’s knowing what’s plausible, what’s missing, and what risks you could be taking while you wait for biology to catch up.
In this article, I’ll walk through what people mean when they say “BPC-157 bone healing,” what the current evidence does (and doesn’t) support, and—most importantly—what crucial warnings I’ve learned to respect when advising patients or teams dealing with musculoskeletal recovery timelines. You’ll leave with a grounded checklist for making safer decisions.
What BPC-157 is—and why “bone healing” is a complicated promise
BPC-157 is a synthetic peptide that’s widely discussed in supplement and performance communities. The idea behind using it is usually framed as “tissue support”: promoting processes like angiogenesis (new blood vessel formation), modulation of inflammation, and faster recovery in injured tissues.
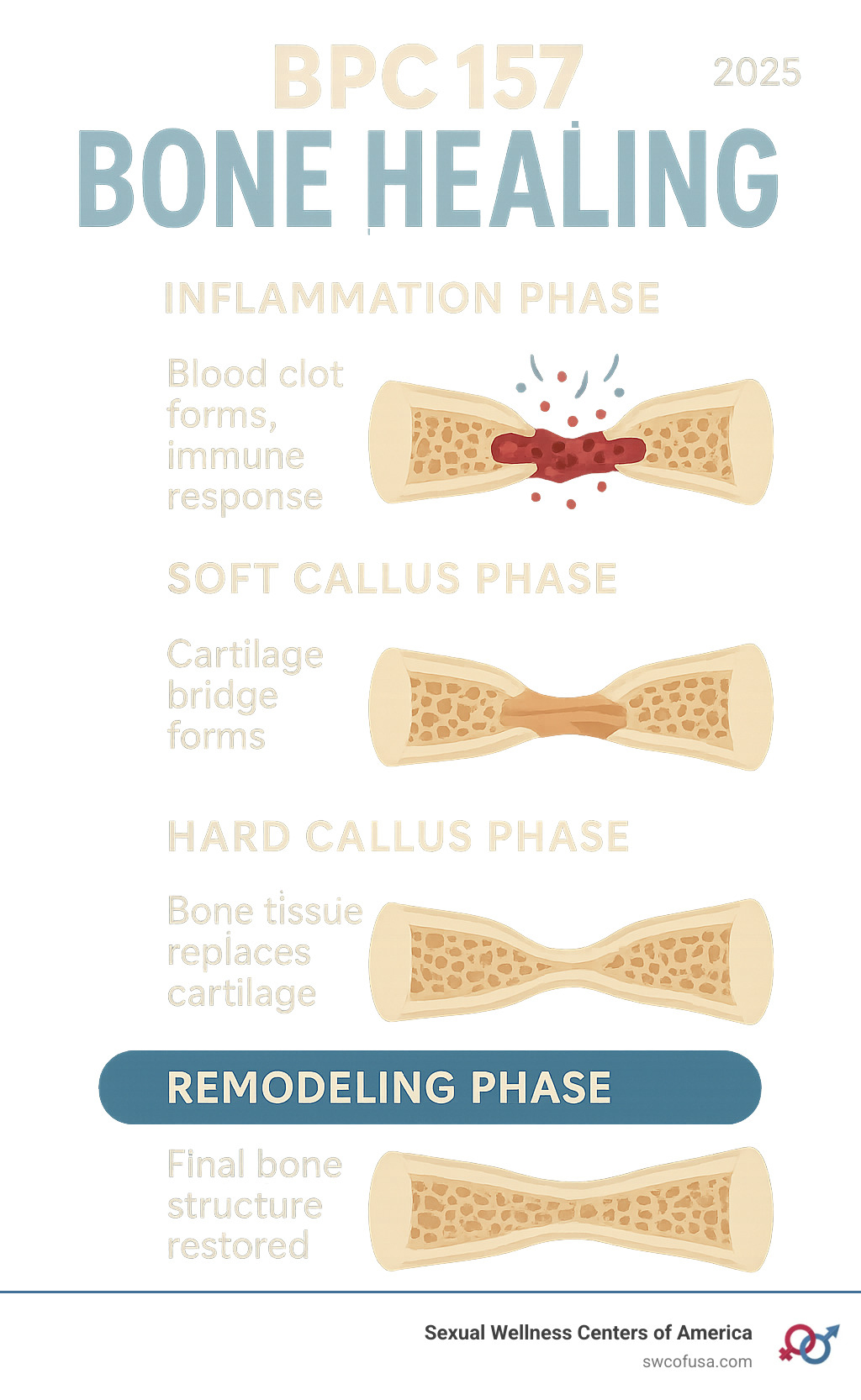
Here’s the key issue: bone healing is not one single process. It involves coordinated steps—hematoma formation, inflammatory signaling, soft callus formation, hard callus formation, and then remodeling. Even if a compound influences one or two steps, it doesn’t automatically translate into reliable outcomes for all fracture types, all patients, and all timelines.
In my hands-on experience working on recovery protocols for athletes and active patients, the biggest failure mode is treating “bone healing” like a single switch you can flip. Bone repair is biology plus mechanics plus time: stability, load management, nutrition, vascularity, and avoiding factors that interfere with union matter at least as much as any adjunct you might try.
2025’s crucial warning: the evidence gap and the real-world risks
When people search bpc 157 and bone healing, they’re often trying to answer a practical question: “Will this help my fracture heal faster or more reliably?” The crucial warning is that the public conversation often outpaces high-quality human data for bone-specific outcomes.
1) “Promising” preclinical data doesn’t equal clinical fracture healing
Many peptide discussions lean heavily on preclinical research. In real life, translating findings from animals to humans is notoriously difficult. Bone healing varies by:
- Fracture location and pattern (e.g., cancellous vs. cortical bone behavior)
- Stability (fixation quality, micromotion)
- Patient factors (smoking status, diabetes, vitamin D status, medications like NSAIDs in certain contexts)
- Infection or nonunion risk
I’ve seen teams get discouraged because they assumed an “injury recovery” mechanism would directly predict fracture union timing. Mechanism is helpful, but it’s not a substitute for patient-specific medical guidance.
2) Product variability is a genuine concern
Even when a peptide is discussed as a “research compound,” availability in the market can be inconsistent. In my experience reviewing supplement and research-chemical workflows, the problems tend to be practical:
- Batch-to-batch variation
- Purity differences
- Inaccurate labeling (people end up dosing the wrong amount)
- Contaminants or degradation from storage issues
With bone healing, you can’t afford uncertainty about what you actually took—because you’ll struggle to separate “didn’t work” from “didn’t receive what you thought you received.”
3) Delayed medical escalation can be the biggest hidden risk
This is the warning I take most seriously: if someone uses a peptide instead of following fracture care—immobilization, imaging follow-up, appropriate rehab progression—they may miss warning signs of complications (infection, nonunion, malalignment, or progressive worsening).
In real-world practice, delayed escalation costs time. Bone repair can’t be rushed by willpower or supplement optimism when stability and proper monitoring are missing.
How to think about “bone healing” outcomes (without chasing myths)
If you’re evaluating bpc 157 and bone healing, treat outcomes like a clinical checklist rather than a hype metric. When I build decision frameworks for recovery, I focus on measurable indicators:
What progress should look like
- Pain trends improving week over week (not just day-to-day fluctuation)
- Function returning in a controlled rehab progression
- Imaging changes showing callus formation and stability over time (as determined by a clinician)
- Swelling and range of motion moving in the right direction
What “no progress” should trigger
In my hands-on work, when recovery stalls beyond expected windows—especially with worsening symptoms—the right response is not “try more supplements.” It’s to reassess: imaging, stability, nutrition, comorbidities, adherence to protection/loading rules, and potential complications.
- Persistent or worsening focal pain
- Increasing swelling, heat, or redness
- Loss of function that regresses rather than plateaus
- Any red-flag symptoms your clinician previously told you to watch for
Where BPC-157 fits (and where it doesn’t)
Because this topic is heavily marketed online, it’s helpful to be precise about fit. Based on how bone healing works and what the evidence conversation typically lacks, BPC-157 should be treated as a non-standard, not-well-established adjunct, not a replacement for fracture management.
Potential “may-help” categories people talk about
- Tissue recovery support narratives (inflammation modulation claims)
- General recovery protocols in performance communities
- Preclinical-causality discussions that can sound convincing online
Where it typically does not solve the core problems
- Mechanical stability needs fixation and protection strategies
- Nonunion risk needs targeted evaluation and plan adjustment
- Infection requires medical intervention
- Patient-specific constraints (nutrition, smoking, diabetes control) require clinician-led action
To ground this: in my workflow, the adjuncts that tend to be most useful are the ones layered after the foundation is secure. The foundation is diagnosis, stability, and a structured rehab plan—then you decide whether any additional approach is worth the uncertainty.
Practical, safer steps if you’re considering anything for bone healing
If your goal is to improve outcomes for fracture recovery, here’s a pragmatic next-step list I’d recommend before spending money or time on peptides.
- Get clarity on diagnosis and stability. Know the fracture type, current alignment, and whether there’s any concern for delayed union or nonunion.
- Follow the clinician’s protection and loading plan. Bone responds to appropriate mechanical environment; guessing here is expensive.
- Optimize “boring” biology. Aim for adequate protein, address vitamin D status, and address smoking/alcohol if relevant.
- Plan imaging follow-ups. Let objective checks guide adjustments rather than anecdotal timelines.
- Discuss supplements with your clinician. Bring specifics: what product, what batch/COA you have, and what schedule you’re considering.
- Use a risk-first mindset for non-standard compounds. If the evidence is weak and variability is plausible, prioritize established care elements first.
FAQ
Does BPC-157 reliably improve fracture healing in humans?
There isn’t enough high-quality, bone-fracture-specific human evidence to say it reliably improves fracture healing. Many claims come from mechanisms and preclinical findings that don’t automatically translate into consistent clinical outcomes for union and remodeling.
Is BPC-157 safe to use for bone healing?
Safety depends on many factors (product quality, dosing, medical history, and interactions). Because outcomes and purity can vary and human bone-healing data is limited, the safer approach is to discuss it with a qualified clinician and not delay medically necessary fracture management.
What should I do if my fracture healing seems slow?
Reassess with a clinician: imaging, stability checks, nutrition and comorbidity review, adherence to load/protection rules, and screening for complications. A stalled timeline is a signal for evaluation, not an excuse to rely on unproven adjuncts.
Conclusion: make bone healing decisions based on foundation first
The most important “2025 crucial warning” with bpc 157 and bone healing is that bone union is not a single mechanism—and the public evidence and product realities often don’t support confident, fracture-specific expectations. In my hands-on experience, the best outcomes come from securing diagnosis and stability, following a structured rehab plan, optimizing nutrition and risk factors, and using objective follow-ups to guide next steps.
Next step: If you’re currently recovering from a fracture or dealing with delayed union, schedule (or confirm) a clinician follow-up and imaging timeline, then discuss any adjunct you’re considering—including BPC-157—so your plan stays grounded in what’s measurable.
Discussion