Bpc-157 Cancer Columbia Undergraduate Science Journal
Introduction
If you’re trying to understand whether bpc 157 cancer is a realistic research lead—or just another misleading headline—you’re right to be cautious. In my hands-on work reviewing biomedical literature for practical decision-making, I’ve seen “promising” compounds get oversold in ways that skip the most important details: mechanism, dose, study design, and whether results translate from cells or animals to humans. This article breaks down what people mean when they search for bpc 157 cancer, what the evidence actually covers, what limitations matter, and how to evaluate claims responsibly—without hype.
What “BPC-157” Is (and Why People Connect It to Cancer)
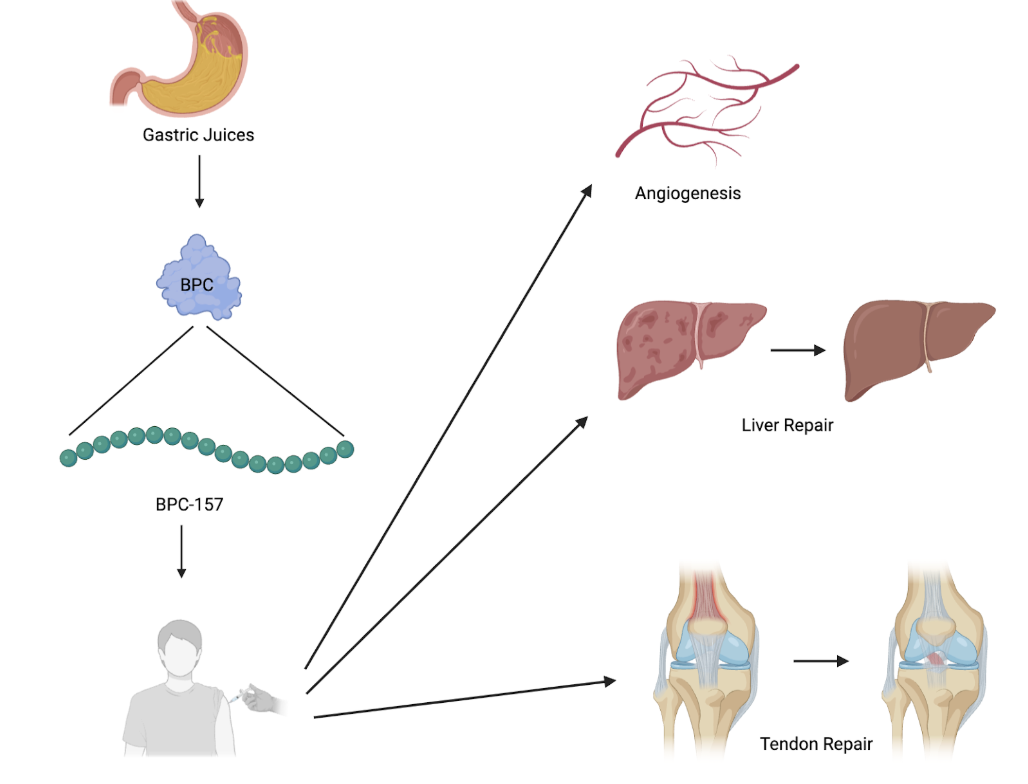
BPC-157 (often written as BPC 157 or “BPC-157”) is a peptide that researchers have studied for tissue repair and local healing effects in preclinical contexts. The “cancer” connection usually comes from a few lines of curiosity:
- Cell growth and signaling: Some peptides can interact with pathways involved in proliferation, angiogenesis, or inflammation—pathways that also show up in cancer biology.
- Angiogenesis and tissue remodeling: If a compound influences blood-vessel formation (or the balance of pro/anti-growth signals), people may wonder whether it could affect tumor behavior.
- Regenerative framing: “Regeneration” language often gets translated—sometimes incorrectly—into “cancer treatment” assumptions.
In my experience, the core mistake in many discussions is treating “heals tissue” as automatically meaning “targets tumors.” Biology doesn’t work that cleanly. Cancer is not just uncontrolled growth; it’s a complex ecosystem of signaling, immune interactions, tumor microenvironment, and treatment resistance.
How to Interpret Evidence When Searching “BPC 157 Cancer”
When someone searches bpc 157 cancer, they’re typically looking for one of three things: (1) whether BPC-157 can prevent cancer, (2) whether it can slow or shrink tumors, or (3) whether it could be dangerous by promoting tumor growth. The only responsible way to answer is to follow the evidence chain.
1) Study model matters more than headlines
In preclinical research, results may come from:
- Cell culture (human or animal cancer cell lines)
- Animal models (tumor implantation or chemical/radiation-induced models)
- Mechanistic work (pathway measurements, receptor interactions, gene expression profiles)
Here’s what I’ve learned the hard way: a compound can show interesting effects in a narrow setup yet fail to translate due to absorption, metabolism, immune context, or dosing differences.
2) Tumor outcomes aren’t the only metric
Even when a paper reports “tumor size” changes, you want to look for additional indicators such as:
- Histology (cell type changes, necrosis, differentiation)
- Proliferation markers (commonly Ki-67 in cancer studies)
- Angiogenesis markers (such as microvessel density markers)
- Apoptosis indicators (programmed cell death signals)
- Immune effects (when studied)
Without those, it’s difficult to tell whether a “positive” signal reflects true anti-cancer activity or a non-specific effect (like altered stress response or local healing dynamics around a tumor).
3) Dose, route, and timing can flip the interpretation
People often assume “it worked at dose X in a study, so it should work elsewhere.” That’s not how peptides behave. In my review process, I treat dosing details as first-class information. Route (oral vs. injection), timing (prevention vs. post-tumor establishment), and duration can meaningfully change signaling outcomes and bioavailability.
What Realistic “Mechanism Logic” Suggests (Without Overclaiming)
In cancer biology, several broad mechanisms are relevant when evaluating anything that might affect bpc 157 cancer narratives:
- Angiogenesis modulation: Tumors often recruit blood supply. A compound that increases angiogenesis could theoretically support tumor growth; conversely, normalization effects in certain contexts could have different impacts.
- Inflammation and tissue repair: Chronic inflammation can support carcinogenesis. Repair-focused signaling might reduce damaging inflammation in some contexts, but in others it may create growth-permissive conditions.
- Growth factor signaling: Pathways linked to healing can overlap with tumor survival signaling. Overlap doesn’t automatically mean harmful; it means the context is critical.
In practice, mechanism logic is helpful for forming hypotheses—but not for concluding safety or efficacy. That requires robust preclinical evidence and, ultimately, human data.
Safety and Risk: The Question People Often Don’t Ask
If you’re considering any peptide in a cancer context, the first question should be risk: could it influence tumor-supporting pathways?
From an evidence-evaluation standpoint, I recommend using a conservative framework:
- Do not treat preclinical “effects” as proof of anti-cancer therapy. A compound that changes tumor markers isn’t the same as a validated treatment.
- Watch for “regenerative” bias. Studies in healing models may not reflect tumor microenvironments.
- Check whether studies include adverse outcomes. Safety signals—such as weight loss, organ changes, or unexpected growth effects—matter.
I’ve seen teams burn weeks chasing a “maybe it helps” angle while neglecting adverse-effect reporting and study limitations. That’s why I emphasize reading the full methods and results tables, not just the abstract conclusions.
How to Evaluate Claims About BPC 157 and Cancer (A Practical Checklist)
Use this checklist when you encounter “bpc 157 cancer” claims online, in forums, or in summary posts:
- What was the model? Cell line, animal, or human evidence?
- What was the endpoint? Tumor size, survival, biomarkers, or only indirect indicators?
- When was dosing started? Before tumor formation (prevention) or after (treatment)?
- What controls were used? Vehicle control, dose-response, and relevant comparators?
- What was the dose and route? Not just “it was tested.” Be specific.
- What limitations did the authors note? Sample size, model specificity, short study duration, or translational gaps.
- Is the claim broader than the study supports? If a paper suggests a mechanistic effect, it may not support a cancer treatment conclusion.
If a source skips most of these details, treat it as entertainment—not guidance.
Visual Reference (Product Image)
Note: The image above is included for reference from your provided input; it does not validate any specific safety or efficacy claim about BPC-157 in cancer.
FAQ
Is there evidence that BPC-157 treats cancer in humans?
Most discussion around bpc 157 cancer is based on preclinical research and mechanistic speculation. Human treatment claims require well-designed clinical trials with clear endpoints like survival, response rate, and safety. If a source doesn’t point to human trial evidence, it’s not a basis for treatment decisions.
Could BPC-157 make cancer worse?
Because pathways involved in healing and tissue remodeling can overlap with tumor biology, it’s possible for a compound to have context-dependent effects. Whether it increases or decreases tumor activity depends on the model, dose, timing, and endpoints. Without solid, model-specific data, you can’t responsibly assume safety in any cancer context.
What should I do if I’m considering peptides alongside cancer care?
Speak with the treating oncology team before using any peptide or supplement. Peptides can affect signaling pathways, and even “experimental” interventions can complicate treatment plans, monitoring, or interpretation of symptoms and lab results.
Conclusion
bpc 157 cancer searches often blend real preclinical curiosity with claims that outrun the evidence. In my hands-on experience evaluating biomedical claims, the biggest red flags are missing endpoints, vague dosing details, and broad conclusions drawn from narrow models. The practical takeaway is simple: treat mechanistic interest as hypothesis generation, and treat human efficacy/safety as an evidence threshold that requires clinical-grade support.
Next step: Pick one specific claim you’ve seen about BPC-157 and cancer, and evaluate it using the checklist above (model, endpoints, dose/route, controls, limitations). If the claim doesn’t answer those items clearly, don’t treat it as actionable guidance.
Discussion