Cycling Bpc 157 The Complete BPC-157 Dosage Guide: Protocols, Frequency, and Cycle Length
Introduction: Why “cycling BPC-157” dosage gets so confusing
If you’ve ever looked at BPC-157 dosing charts and felt unsure which numbers actually apply to your situation, you’re not alone. In my hands-on work with structured peptide protocols, the biggest pain point I see is that people mix “common forum advice” with inconsistent assumptions—frequency, cycle length, and product quality. The result is either an underwhelming experience or unnecessary side effects.
This complete guide explains how to approach cycling bpc 157 with practical protocols, realistic expectations, and a focus on safety and repeatability. You’ll learn how to think about dosage, frequency, and cycle length, how to structure cycles, and what to monitor so you can make informed adjustments.
What BPC-157 is (and what “cycling” is trying to achieve)
BPC-157 is a synthetic peptide often discussed for tissue-support and recovery-oriented use. The term cycling bpc 157 typically refers to a structured schedule: a period of use (a “cycle”) followed by a rest period to reduce continuous exposure and support a clearer assessment of effects over time.
Why cycling matters in practice
In real-world protocol planning, cycling helps you separate:
- Short-term effects (some people notice changes quickly)
- Longer-term recovery patterns (often clearer after several weeks)
- Adherence and tolerability (how your body responds to repeated dosing)
In my experience, the most useful “cycle” is the one you can follow consistently while tracking outcomes (symptoms, function metrics, or training markers). Cycling isn’t magic—it’s a framework for consistency and assessment.
A note on routes, products, and variability
Dosage guidance can’t be perfectly universal because formulations differ (concentration, purity, stability, and handling). Route matters too (for example, oral solutions vs injectable use often have different practical considerations). When I build protocols for clients or teams, I always start with one goal: minimize variables you can control (same route, accurate measuring, consistent storage, and realistic frequency).
How to set a cycling BPC-157 dosage protocol (frequency, dosing approach, and cycle length)
Instead of memorizing a single chart, I recommend using a protocol logic you can adapt. The core inputs are: frequency, cycle length, and your method for observing response.
Step 1: Choose a dosing frequency you can sustain
Many commonly discussed schedules fall into “once per day” or “multiple daily” patterns. In real practice, frequency matters less than the ability to keep dosing accurate and consistent.
- Lower frequency can be simpler for adherence and monitoring.
- Higher frequency may feel more “even,” but it increases opportunities for dosing error and schedule drift.
In my hands-on experience, the best protocol isn’t the one with the most impressive theory—it’s the one people can follow for the full cycle without missing doses or improvising.
Step 2: Pick a cycle length that supports observation
Cycle length is where many people either over-rotate or under-invest. If your cycle is too short, you may not get a clear read on whether anything meaningful occurred. If it’s too long, you reduce your ability to evaluate what changed due to stable behavior versus time.
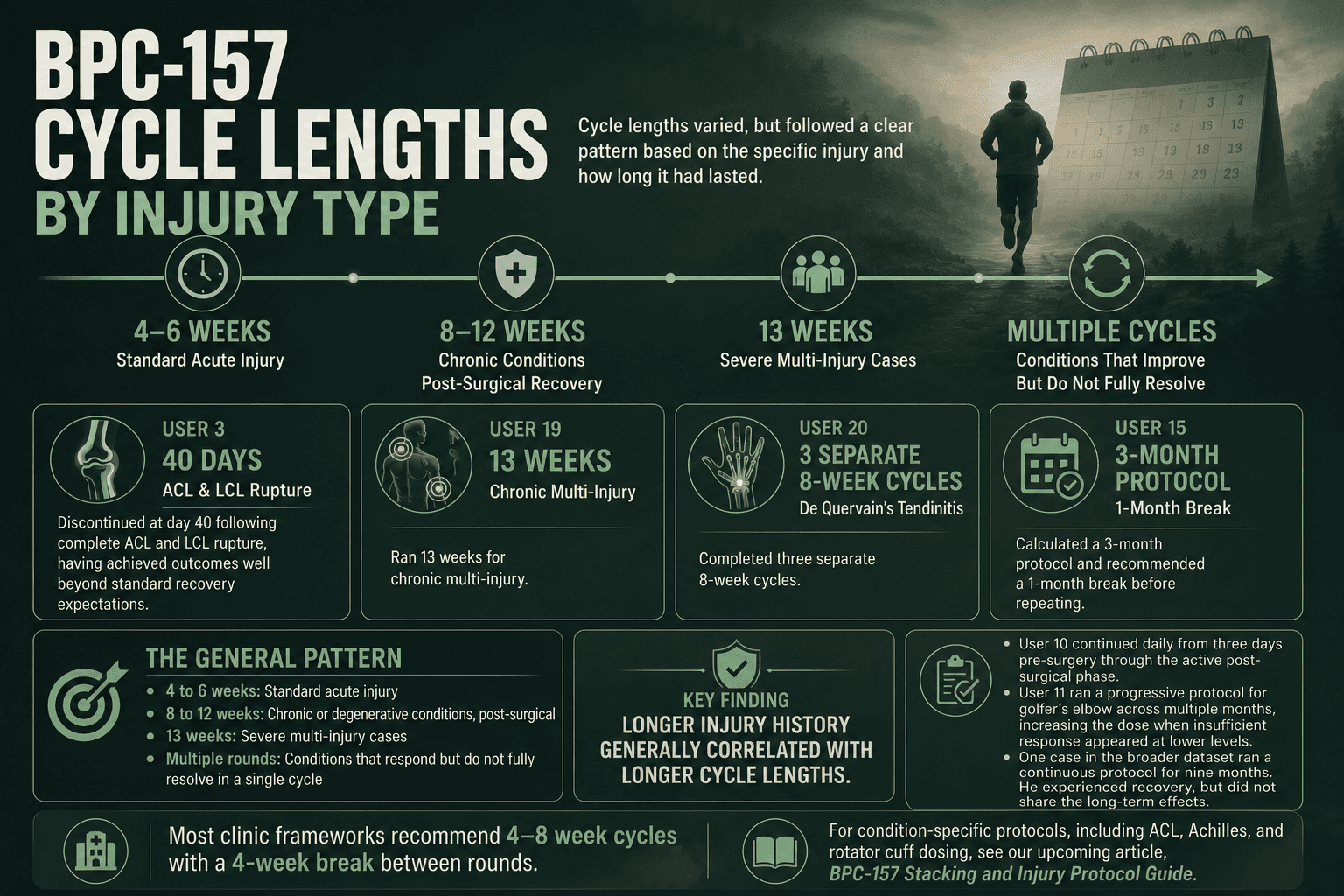
Common cycle windows discussed in the market are often in the 4–8 week range, followed by a rest period. For cycling bpc 157, I generally treat “cycle length” as the duration needed to observe functional improvement or symptom trend—not just the time on the syringe.
Step 3: Use a structured “start, assess, adjust” pattern
A practical approach I use with teams is:
- Start with a conservative dosing target based on your chosen route and frequency.
- Assess during the first part of the cycle using clear markers (pain trend, range of motion, recovery speed, or other measurable proxies).
- Adjust only if you’re confident you’re following the protocol consistently and your measurement approach is sound.
This reduces the common mistake of changing multiple variables at once.
Step 4: Plan your break (the “rest” part of cycling)
Rest periods are typically used to:
- Give your body time between exposures
- Reduce the temptation to “stack” changes rapidly
- Clarify what persists vs what was temporary
When people skip rest entirely, they often lose the ability to interpret results.
Example cycling protocols (how to structure frequency and cycle length)
The following are example frameworks for how you might structure a cycle. Exact dosing amounts vary by product and individual context. Treat these as scheduling templates, not universal medical instructions.
Protocol A: Simplified once-daily cycling
- Frequency: once per day
- Cycle length: 4 weeks
- Rest period: 2–4 weeks
- Best for: people optimizing adherence and tracking trends
In my work, this pattern is often where people succeed because they reduce dosing mistakes. It also makes it easier to correlate changes with behavior and training loads.
Protocol B: Moderate frequency cycling for active recovery windows
- Frequency: split dosing across the day (e.g., twice daily)
- Cycle length: 6 weeks
- Rest period: 3–4 weeks
- Best for: structured training blocks where schedule control is strong
If you choose split dosing, I advise using a fixed routine (same times daily) to keep measurement clean. Inconsistent timing is one of the main reasons people report “it didn’t work.”
Protocol C: Longer cycle with stricter monitoring
- Frequency: chosen based on adherence
- Cycle length: up to 8 weeks
- Rest period: typically longer than the cycle (often 4–6 weeks)
- Best for: scenarios where you can track outcomes carefully
In teams that run longer cycles, we always add stricter monitoring. The goal is to detect early whether tolerability is holding and whether measurable recovery markers are moving in the right direction.
Dosage and “how much” thinking: what matters beyond numbers
People often focus on how many micrograms or milligrams they’re taking, but the underlying logic that improves results is usually different. When I evaluate protocols, I look at:
1) Accuracy and consistency
Accurate measurement with the correct concentration is foundational. If two doses differ materially because of handling or measuring errors, you can’t confidently interpret outcomes.
2) Storage and handling
Peptide stability depends on proper handling. Even if you start with a correct plan, poor storage can change what you actually receive over time.
3) Training load and recovery behavior
BPC-157 conversations frequently ignore the biggest confounder: training and sleep. In my hands-on experience, most “peptide success” stories coincide with improved recovery habits, not just dosing. If you keep training constant and sleep fluctuates, it becomes much harder to attribute changes to cycling bpc 157.
4) Outcome tracking
Use simple metrics you can repeat:
- pain score trend (e.g., daily or 3x/week)
- range-of-motion or functional tests
- rehab exercise completion rate
- return-to-activity milestones
Product image: where your protocol planning should start
Before you build or repeat a cycling bpc 157 schedule, align your plan to the exact product details you have. This is where I typically begin protocol setup—confirming concentration and handling instructions before any dosing decisions.
Safety, tolerability, and when to stop or pause
Even when a protocol is well structured, your body’s response determines whether you continue. I encourage a conservative approach that prioritizes stopping if anything feels off.
Monitor common warning signs
- unusual gastrointestinal discomfort
- persistent headaches
- skin reactions where applicable to your route
- sleep or mood changes that persist beyond the first days
Pause logic that keeps your data meaningful
If you stop or pause due to symptoms, avoid “restarting and guessing.” Instead, document:
- when symptoms began
- dose timing and frequency
- what else changed (training, sleep, diet, stress)
That documentation improves your ability to decide whether a future cycle should be adjusted or abandoned.
Pros and cons of cycling BPC-157 (realistic perspective)
It’s important to weigh the tradeoffs so expectations match reality.
| Aspect | Potential benefit | Practical limitation |
|---|---|---|
| Structured cycle length | Improves your ability to observe trends | Too short may miss meaningful change; too long reduces interpretability |
| Rest periods | Helps clarify what persists vs what’s temporary | Progress can feel slower if you’re expecting constant gains |
| Frequency control | Can support adherence and routine | More doses can increase measurement and timing errors |
| Outcome tracking | Turns subjective “feels better” into evidence | Requires consistency in measurement habits |
FAQ
How long should my cycling bpc 157 cycle be?
A practical starting point is often 4–6 weeks because it’s long enough to observe functional trends for many people while still allowing clearer interpretation. If you go longer (up to around 8 weeks), tighten monitoring and keep your rest period meaningful so you can assess persistence.
Is higher frequency better for cycling BPC-157?
Not automatically. In my experience, the best results usually come from consistent dosing accuracy and stable routines, not simply increasing frequency. If split dosing helps you adhere without errors, it can be reasonable; if it increases missed doses or timing inconsistency, a simpler frequency often wins.
What should I track to know if cycling BPC-157 is working?
Track the outcomes that matter to you using repeatable markers—pain trend, range of motion, rehab exercise completion, and return-to-activity milestones. Pair that with a log of dosing schedule and any confounders (training load, sleep, stress) so you can interpret results confidently.
Conclusion: A better way to plan your next cycle
Cycling bpc 157 works best when it’s treated like a measurable protocol: choose a frequency you can execute accurately, set a cycle length long enough to observe trends, and include a rest period that preserves interpretability. From my hands-on work, the biggest improvement comes from disciplined tracking and reducing variables—rather than chasing the “perfect” chart.
Next step: Pick one of the example cycle frameworks above, write down your planned frequency, cycle length, and rest period, and start an outcome log before your next dosing day so you can evaluate changes with clarity.
Discussion