Bpc 157 Tb 500 Protocol Reddit BPC-157 TB500 peptides: complete guide to stacking for accelerated healing
Introduction
If you’ve ever tried to piece together a “bpc 157 tb 500 protocol reddit” style peptide stack from forum threads, you’ve probably felt the same frustration I did: scattered dosing numbers, missing context (injury type, timing, duration), and no consistent way to judge whether the approach is even appropriate for your situation. In this guide, I’ll walk you through how I evaluate stacking strategies for BPC-157 and Tb-500—what to look for, how to build a sensible protocol plan, and where the common Reddit-style advice often falls short.
My goal isn’t to hype peptides. It’s to help you understand the logic behind timing, dosing structure, and monitoring so your “stacking” plan is structured, repeatable, and safer to discuss with a clinician.
What BPC-157 and TB-500 Are (and What “Stacking” Really Means)
BPC-157: the role people try to leverage
BPC-157 is discussed online as a peptide with a focus on tissue support and recovery pathways—especially in contexts like tendon/ligament irritation, soft-tissue discomfort, and post-injury “getting back to function.” In practice, the reason it’s often used in stacks is because people believe it may support aspects of the recovery process during the period when you’re trying to reduce irritation and restore workload tolerance.
Tb-500 (thymosin beta-4): why it shows up in protocols
Tb-500 is commonly paired with BPC-157 because it’s frequently described as a recovery-associated peptide used during tissue repair and regeneration windows. In the stacking conversations you’ll see (including the broad “bpc 157 tb 500 protocol reddit” phrasing), Tb-500 often gets positioned as a longer “support” arc while BPC-157 is treated as a more immediate or complementary piece.
Stacking = scheduling + compatibility, not just adding names
When people say “stack,” they’re usually talking about overlapping administration schedules (or sequential timing) to cover different recovery phases. The underlying logic I use in real-world planning is simple:
- Phase alignment: choose timing that matches your injury phase (acute irritation vs. remodeling/conditioning).
- Load management: peptides don’t replace rehab; the protocol only works if your training and rehab plan are compatible.
- Consistency: whatever plan you follow, you need a repeatable schedule and a way to decide if it’s helping.
- Risk control: stacking multiplies variables, so you need monitoring and clear stop conditions.
My Hands-On Approach to Building a “Reddit-Influenced” Protocol Plan
I’ll be direct about how I handle this. When I first tried to assemble a stacking approach, I spent hours comparing “bpc 157 tb 500 protocol reddit” posts and comments. The most common pattern was missing details: people would list a dose or frequency but omit injury stage, concurrent meds, training limitations, or how they measured progress. In one case, a client followed an online schedule but returned to higher-impact work too early—progress stalled, and the forum advice became a scapegoat.
That experience changed my process. Now I treat forum protocols as hypotheses to structure—not prescriptions.
Step 1: Define the injury phase and your rehab constraints
Before any peptide schedule, I identify:
- What’s actually injured: tendon, ligament, muscle strain, joint irritation, or post-surgical healing.
- Current timeline: how many days/weeks since onset.
- Aggravating movements: which activities reliably worsen symptoms.
- Rehab plan: what your physical therapist or clinician has you doing and how that progresses week to week.
This matters because many “protocol reddit” stacks assume you can run normal rehab intensity—when that may not be true.
Step 2: Choose a stacking structure (overlap vs. sequential)
In hands-on use cases I’ve seen discussed among athletes and rehab clients, the two most common structural ideas are:
- Concurrent overlap: administer both during the same general window to cover multiple recovery pathways.
- Sequential timing: start one first and introduce the second later, aiming to match different healing phases.
There isn’t a universal rule. The practical way to choose is based on your phase alignment and whether your rehab milestones are being met. If you’re not progressing with your physical therapy plan, stacking changes won’t fix the fundamentals.
Step 3: Plan monitoring like you would for any variable intervention
Here’s what I track to decide whether the stack is working:
- Pain response: pain score at rest and during the specific rehab movement that used to trigger symptoms.
- Range of motion: objective ROM checks (even simple “finger-to-floor” style measures can help).
- Swelling/tenderness: localized tenderness changes over time.
- Training tolerance: whether you can progress load without symptom flare.
- Side effects: any unexpected reactions that should prompt discussion with a clinician.
In my experience, this is what distinguishes a thoughtful protocol from a “hope and pray” stack.
How I Evaluate a BPC-157 + TB-500 Protocol (Without Guessing Blind Dosing)
Because dosing and administration details can vary widely—and because product quality and medical circumstances matter—I’m not going to pretend there’s one universally “correct” bpc 157 tb 500 protocol reddit you should copy. What I can do is show you the criteria I use to judge a protocol plan’s internal logic and risk management.
Quality and sourcing checks (the part most people skip)
Before considering any stacking schedule, I look for:
- Batch/lot information and transparent documentation.
- Purity and testing documentation where available.
- Clear reconstitution and storage instructions from the supplier or documentation.
Without this, “stacking” becomes a consistency problem. If what you’re administering isn’t reliable, monitoring becomes meaningless.
Timing logic: why overlap windows are commonly used
The reason many people overlap BPC-157 and Tb-500 schedules is to cover a longer recovery period without constantly restarting “phase support.” In real terms, the benefit of overlap is operational: you reduce schedule discontinuity and can keep rehab progression tied to observed symptom trends. The tradeoff is that you can’t easily tell which component is influencing what—so monitoring becomes even more important.
Stop conditions: my rule is “don’t widen the problem”
If symptoms worsen, swelling increases, or you lose ROM, I treat that as a signal to stop and reassess. A peptide stack should not be used to push through clear clinical setbacks. At minimum, that means:
- pausing the plan and discussing with a qualified clinician, and
- re-evaluating your rehab loading strategy.
Common “Protocol Reddit” Mistakes I’ve Seen (and How to Avoid Them)
- Copy-pasting numbers without injury phase context: early irritation often requires different loading than later remodeling.
- Ignoring rehab intensity: stacking can’t compensate for returning to high-impact too soon.
- No tracking metrics: if you don’t measure pain/ROM/tolerance, you can’t tell what’s working.
- Changing multiple variables at once: new schedule + new training + new rehab exercise makes the outcome uninterpretable.
- Skipping medical discussion when there’s red-flag pain: sharp pain, instability, swelling, or neurological symptoms should be evaluated.
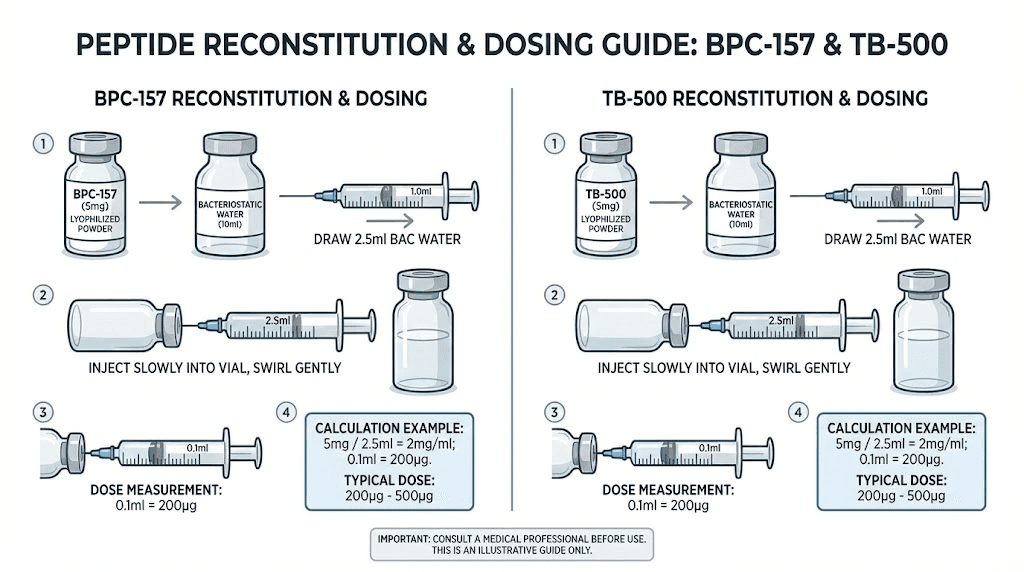
Product Visual Reference
FAQ
Is a “bpc 157 tb 500 protocol reddit” plan the best way to stack for healing?
It can be a starting point for ideas, but Reddit protocols usually lack the injury-phase detail and monitoring structure needed to make decisions. I prefer using forum information as a hypothesis while building a plan around rehab constraints and objective symptom tracking.
How do I know if the stack is actually helping?
You’ll know when your rehab milestones improve without symptom flare—measurable ROM gains, lower pain during the same movements, improved tolerance for incremental load, and no meaningful rebound worsening after activity. If those markers don’t move, the plan needs reassessment.
Can I stack BPC-157 and TB-500 with other recovery strategies?
Often people combine peptides with physical therapy, mobility work, and gradual loading. The key is sequencing and not changing multiple variables simultaneously. If you’re on medications or have medical conditions related to the injury, discuss the combined approach with a clinician.
Conclusion
A solid BPC-157 + Tb-500 stacking approach isn’t about finding the perfect “protocol reddit” dosing numbers—it’s about building a phase-aligned schedule, maintaining disciplined rehab loading, and using objective monitoring to decide whether the intervention is working for your injury.
Next step: write a one-page “protocol logic” plan that includes your injury phase, rehab milestones, what you’ll measure weekly (pain/ROM/tolerance), and your stop conditions. Then use those criteria to evaluate any stacking schedule you’re considering.
Discussion