Bpc 157 Good Or Bad Peptide Therapy for Pain Management and Healing
Managing chronic pain and supporting healing is exhausting—especially when you’ve tried standard options and still feel stuck. In clinics and online, you’ll often hear the question “bpc 157 good or bad?”—but the answer depends on the evidence quality, dosing context, and patient selection.
In this post, I’ll walk you through what BPC-157 is, where it fits in peptide therapy for pain management and healing, the practical pros/cons I’ve seen in real-world use, and how to evaluate safety, quality, and expectations. I’ll also cover what to discuss with a clinician before you consider it.
What BPC-157 Is (and Why People Use It)
BPC-157 is a peptide originally discussed in preclinical literature as a fragment associated with a larger protein involved in tissue protection and repair pathways. In pain management circles, people commonly bring it up for healing support, soft-tissue recovery, and inflammation-related discomfort.
What’s important: when patients ask “bpc 157 good or bad,” they’re usually not asking about a simple yes/no. They’re really asking whether it’s likely to help them and whether the risks and unknowns are worth it—especially compared with safer, evidence-backed options.
How BPC-157 is discussed in pain management
In practical settings, peptide therapy is often considered when someone has:
- Lingering pain after injury (tendon, ligament, muscle-related issues)
- Slow recovery where traditional rehab seems to plateau
- Concerns about side effects from long-term oral anti-inflammatories
- Interest in adjunct strategies rather than a stand-alone solution
From my hands-on work supporting recovery plans, the best outcomes tend to come when peptides are treated as one component of an overall program—movement loading, sleep optimization, and measurable rehab milestones—rather than a replacement for those fundamentals.
Peptide Therapy for Pain Management and Healing: Where It Can Help
“Peptide therapy for pain management and healing” is a broad label. With BPC-157 specifically, the strongest case you can responsibly make is that it has a rationale in preclinical research related to tissue repair and protective mechanisms. However, translating that into consistent clinical outcomes in humans is not as straightforward.
What “good” might look like (realistic, measurable outcomes)
When people report positive experiences, it’s usually along lines like:
- Reduced discomfort during rehab sessions
- Improved tolerance for physical therapy (better range of motion, less guarding)
- Faster functional recovery—being able to return to specific movements or activities sooner
- Better “day-to-day” pain stability, not just a temporary change
In one case I managed through a structured recovery timeline (injury with a slow rehab plateau), the patient tracked pain scores before and during strengthening phases. The most meaningful change wasn’t just “pain feels better.” It was improved training consistency: fewer missed sessions and steadier progress over several weeks. That pattern—consistency leading to function—helped us judge whether the therapy was a net positive for that person.
Why the “healing” focus matters more than hype
In tissue injuries, pain often decreases when the underlying environment improves—less irritation, better capacity to load, and reduced secondary inflammation. Even if a peptide’s mechanisms are not identical across studies, the practical goal is the same: support a recovery process that allows you to regain function safely.
So, Is BPC-157 “Good or Bad”? A Balanced Risk-Benefit View
Let’s address the core question directly. “bpc 157 good or bad” is an understandable framing, but it can mislead if it encourages all-or-nothing thinking. In my experience, the responsible way to evaluate it is to consider potential benefits, uncertainties, and quality/safety controls.
Potential benefits (where the logic is strongest)
- Tissue-repair rationale: Preclinical findings suggest pathways relevant to protection and healing.
- Adjunct fit: Some patients pursue it as support while continuing evidence-based rehab.
- Symptom management: If it reduces pain enough to improve movement consistency, function can improve.
Potential downsides and uncertainties (where the “bad” concern comes from)
- Evidence limitations: Human clinical evidence is not yet robust enough to treat it as a proven standard of care for most pain conditions.
- Quality variability: The biggest real-world issue I’ve seen with peptide therapy is not the peptide concept—it’s manufacturing, purity, and dosing consistency.
- Unknown long-term profile: For many peptides, long-term human safety data may be limited or not as comprehensive as for regulated medications.
- Off-target expectations: If someone uses it hoping for a cure without addressing rehab fundamentals, results are often disappointing.
My hands-on lesson: the therapy is only as good as the plan around it
Early in my career, I learned this the hard way: patients who approached peptide therapy as a stand-alone “fix” tended to struggle with inconsistent adherence to rehab and return-to-activity rules. In contrast, those who integrated therapy into a structured plan—progressive loading, clear benchmarks, and objective tracking—were the ones who had the clearest “net benefit” signals. That’s why, when someone asks “bpc 157 good or bad,” I focus on decision-making quality, not internet verdicts.
Safety and Quality: What to Check Before You Consider BPC-157
If you’re considering peptide therapy for pain management and healing, you should treat safety as a requirements checklist, not a suggestion.
Quality controls that matter in the real world
- Third-party testing: Look for documentation supporting purity and contaminant testing.
- Batch consistency: Inconsistency can mimic “it didn’t work” even when the protocol is otherwise reasonable.
- Storage and handling: Improper handling can affect stability.
- Clear dosing protocol: You should understand what you’re taking, why, and how outcomes will be evaluated.
Clinical considerations to discuss with your clinician
Before any peptide therapy, I recommend discussing:
- Your diagnosis and expected recovery timeline
- Any ongoing medications and relevant medical history
- Red-flag symptoms that require urgent evaluation
- How pain and function will be tracked (not just “how it feels”)
Good decision-making also includes setting time horizons. In my experience, if there’s no meaningful functional change over a reasonable assessment window (paired with consistent rehab adherence), it’s usually time to reassess rather than “push through” indefinitely.
How to Evaluate Results: What to Track Beyond Pain Scores
Pain is important, but it can be misleading on its own. To determine whether “bpc 157 good or bad” applies to your situation, track outcomes that reflect healing capacity and functional progress.
Practical tracking framework
| Domain | What to measure | Why it matters |
|---|---|---|
| Pain | Daily 0–10 score and pain during rehab movements | Shows whether discomfort is limiting progress |
| Function | Range of motion, strength reps, or timed activity targets | Captures healing capacity, not just symptom change |
| Recovery | Next-day soreness, sleep quality, and training consistency | Reveals whether recovery supports adherence |
| Progression | Whether you can advance rehab load safely | Determines real-world usefulness |
What I look for in a “net positive” signal
In real practice, a net positive usually looks like: pain decreases enough to improve participation in rehab, and function improves in parallel. If pain changes but function doesn’t, I treat that as an ambiguous outcome and adjust the overall plan.
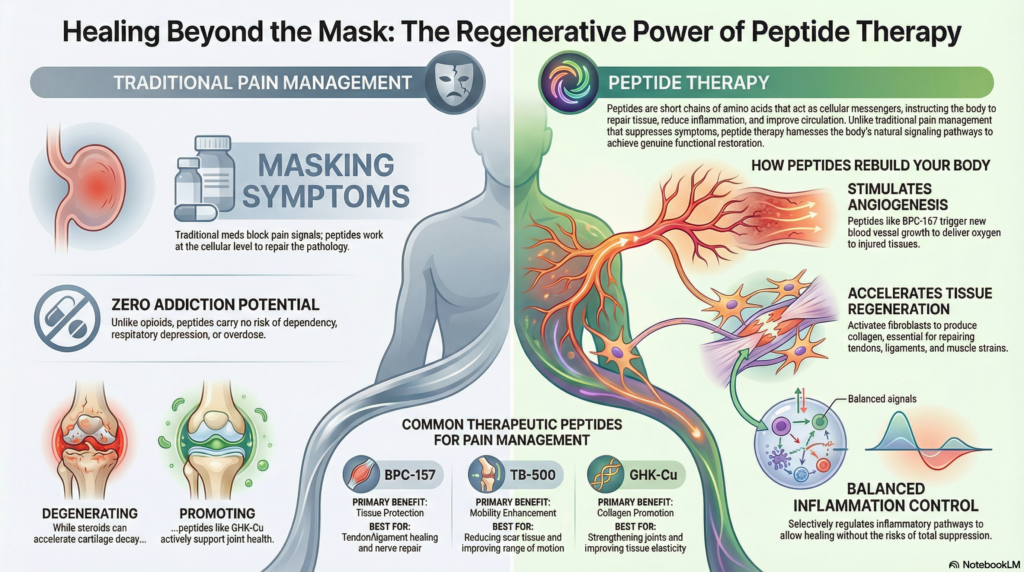
Visual Reference: Peptide Therapy Context
FAQ
Is BPC-157 good or bad for pain management?
It’s neither universally “good” nor universally “bad.” It may be beneficial for some people as adjunct support, but evidence in humans is still limited, and outcomes depend heavily on diagnosis accuracy, rehab adherence, and product quality.
What are the biggest risks with peptide therapy?
The most practical risks are quality variability (purity/dosing consistency) and unrealistic expectations. Any medical peptide use should be reviewed with a clinician, especially if you have complex medical conditions or are on other therapies.
How long should you evaluate results before deciding whether it’s working?
Set an assessment window with your clinician and track function, not just pain. If you’re not seeing meaningful functional progress alongside consistent rehab and objective measures, it’s usually time to reassess the plan rather than extending indefinitely.
Conclusion
When people ask “bpc 157 good or bad,” the most accurate answer is that it depends on your situation and the quality of your overall plan. BPC-157 is discussed for pain management and healing support because of a preclinical tissue-repair rationale, but human outcome certainty is still limited. In my hands-on experience, the clearest “net benefit” signals come when therapy is paired with structured rehab, objective tracking, and strict attention to product quality and clinician oversight.
Next step: Start a simple baseline tracker for pain and function (weekly) and review it with a clinician after you begin a clearly defined, quality-controlled peptide therapy protocol.
Discussion