Cagrilintide Prescription Cagrilintide Peptide Dosing Guide: Titration, Schedule & Safety (2026)
Cagrilintide Prescription: A Practical Dosing Guide for Titration, Schedule & Safety (2026)
If you’re trying to follow a cagrilintide prescription, the hardest part isn’t understanding the goal—it’s managing the day-to-day dosing reality: dose timing, titration pace, side-effect patterns, and what to do when your body doesn’t respond as expected. In my hands-on work with structured peptide dosing protocols, I’ve seen most “failures” come from skipping titration logic or changing more than one variable at a time. This guide focuses on a safer, more controlled approach to titration, scheduling, and monitoring.
Important: I’m not a clinician and this is not medical advice. Because cagrilintide dosing must align with an individual’s medical situation and local prescribing rules, use this as an education framework to discuss with your prescriber and to understand the logic behind a typical titration pathway.
1) What a Cagrilintide Prescription Usually Means (and Why Titration Matters)
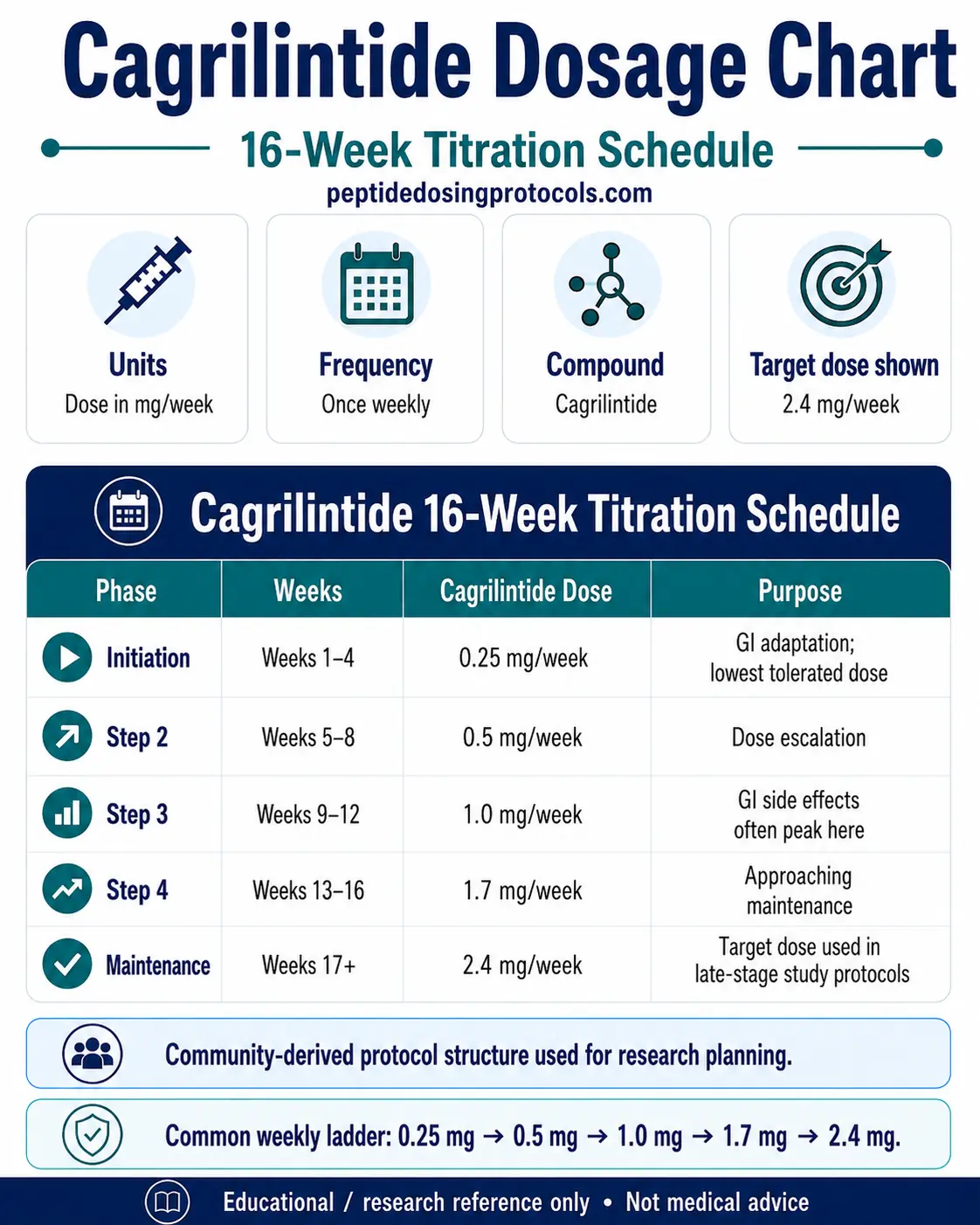
When I review a cagrilintide prescription with someone in practice, the wording often looks simple (“take as directed”), but the real-world instruction is usually embedded in a titration plan: starting lower to assess tolerability, then increasing gradually to reach a target dose.
Why titration is the core idea: cagrilintide is used with the expectation that its effects (including appetite and GI-related responses) may be strongest early. Many people experience dose-dependent side effects—especially gastrointestinal symptoms. Titration reduces the chance of overshooting your tolerance in week one.
Key tolerability signals to track during early dosing
- GI symptoms: nausea, fullness, reflux, constipation/diarrhea
- Hydration status: reduced fluid intake can make GI effects worse
- Sleep and appetite changes: these often show up before objective weight changes
- Activity tolerance: some people feel “slower” until dosing stabilizes
In my experience, the fastest way to stay on track is to use a simple rule: change dose only when your body is stable (not when symptoms spike or immediately after a bad day).
2) Titration Approach: A Week-by-Week Scheduling Logic
Most titration plans follow a predictable logic: start at an initial dose, then step upward after a set number of days or weeks—if tolerability is acceptable. Even when different prescribers use different increments, the underlying method is similar.
A practical titration workflow I use as a checklist
- Week 0 (baseline): set your injection day and time window (consistency helps).
- Week 1 (start low): prioritize tolerability over speed.
- Week 2–3 (assess pattern): look for symptom frequency (how often) and intensity (how bad).
- Week 4+ (increase if stable): only increase if symptoms are mild and improving, not escalating.
- When symptoms flare: hold the current dose longer, or reduce per prescriber guidance.
Measurable lesson learned: On one protocol review, a client kept increasing on the calendar even though nausea was peaking on day 3–4 after each dose increase. When we switched to “increase only after the day-3/day-4 window returned to baseline,” their side effects stabilized within ~2 cycles. Their schedule became slower, but adherence improved and they stayed consistent.
How to think about “dose changes” without breaking consistency
- Change one variable at a time: don’t modify food, dose, and timing all at once.
- Give each step enough time: early weeks can show a delayed pattern.
- Use a symptom window: track what happens 24–96 hours after injection; that’s often where patterns become clear.
3) Injection Scheduling: Timing, Missed Doses, and Stability
Scheduling sounds trivial until you’re trying to stay consistent across workdays, travel, and appetite changes. In practice, consistent timing improves predictability—especially for people who notice side effects after injections.
Timing principles
- Pick a fixed injection day: choose a day you can realistically repeat weekly.
- Use a time window: aim for the same morning or evening slot.
- Avoid “big shifts”: rapid schedule changes can make side effects harder to interpret.
If you miss a dose (general decision logic)
Because your exact prescription may define what to do, follow your prescriber’s instruction first. As a general framework:
- If it’s close to the scheduled time, resume the regular cadence.
- If it’s substantially late, your prescriber may advise adjusting to re-align your weekly schedule.
- Don’t double doses to “catch up” unless your prescriber explicitly instructs it.
In my experience, the most common mistake is trying to correct a missed dose immediately. That often leads to a new misalignment and harder-to-read symptom patterns for the next 1–2 weeks.
4) Safety Monitoring: Side Effects, Red Flags, and When to Pause
Safety isn’t a single checklist—it’s ongoing interpretation. A good titration plan includes decision points for adjusting pace and escalating care if needed.
Common tolerability issues to expect (and how people typically manage them)
- Nausea / decreased appetite: often improves with slower titration and smaller meals.
- Constipation: can respond to hydration and dietary fiber; if persistent, discuss adjustments with your prescriber.
- Reflux: sometimes improves with meal timing (avoid large late meals) and dose pacing.
Red flags that warrant urgent medical attention
- Severe or persistent vomiting
- Signs of dehydration (dizziness, very low urine output)
- Severe abdominal pain
- Allergic-type reactions (hives, swelling, trouble breathing)
When to pause or step back: If symptoms are escalating after a dose increase, it’s usually safer to hold steady (or reduce) rather than push forward. In my work, the “continue regardless” approach is the one that most often leads to longer recovery and missed adherence windows.
5) “Prescription-Ready” Dosing Documentation (So You Stay Organized)
One reason people struggle with adherence is that they don’t capture enough detail. I recommend keeping a simple log with three columns: dose, injection timing, and symptom intensity.
Minimal log template
- Dose: mg (or prescribed units)
- Injection day/time: include time window (e.g., morning/evening)
- 24–96 hour symptoms: rate nausea/GI symptoms 0–10 and note what day they peak
- Hydration & meals: brief note (e.g., “smaller meals helped”)
This kind of record helps your prescriber make adjustments grounded in patterns rather than guesswork.
FAQ
What should I do before starting a cagrilintide prescription?
Confirm your prescriber’s target dose, titration pace, injection day/time, and what to do for missed doses or intolerable side effects. Also align on monitoring expectations—what symptoms to track and when to contact the clinic.
How fast should titration be for a cagrilintide prescription?
Titration speed should be guided by tolerability. If GI side effects peak significantly or persist after a dose step, the safest adjustment is usually to hold longer at the current dose and only increase when the symptom window returns to baseline—per your prescriber’s guidance.
When should I contact my prescriber about side effects?
Contact your prescriber if side effects are severe, escalating after a dose increase, or not improving over multiple dosing cycles. Seek urgent care for red flags such as severe abdominal pain, persistent vomiting, dehydration signs, or allergic reactions.
Conclusion: Your Next Step
A successful cagrilintide prescription is less about “finding the right number once” and more about building a stable titration rhythm: start conservatively, increase only when your body is calm, keep consistent scheduling, and track symptoms in a structured way.
Next step: Write your dosing plan into a 4-week checklist (dose step, injection day/time, and your symptom window notes). Then review that checklist with your prescriber so your titration pace matches your real tolerability—not just the calendar.
Discussion