Bpc 157 For Nerve Pain Peptide Therapy for Pain Management and Healing
Introduction
If you’re dealing with nerve pain—burning, tingling, shooting discomfort that doesn’t follow a simple “muscle strain” pattern—you already know how frustrating it is to find something that helps without adding more problems. In my hands-on clinical work, I’ve seen people go from trialing multiple pain approaches to asking a more targeted question: can bpc 157 for nerve pain support healing pathways and help reduce symptoms? This article breaks down what peptide therapy is, how BPC-157 is commonly used in pain management discussions, where it may fit, and how to think about risks and realistic expectations.
What Peptide Therapy Is (and Why It’s Discussed for Pain)
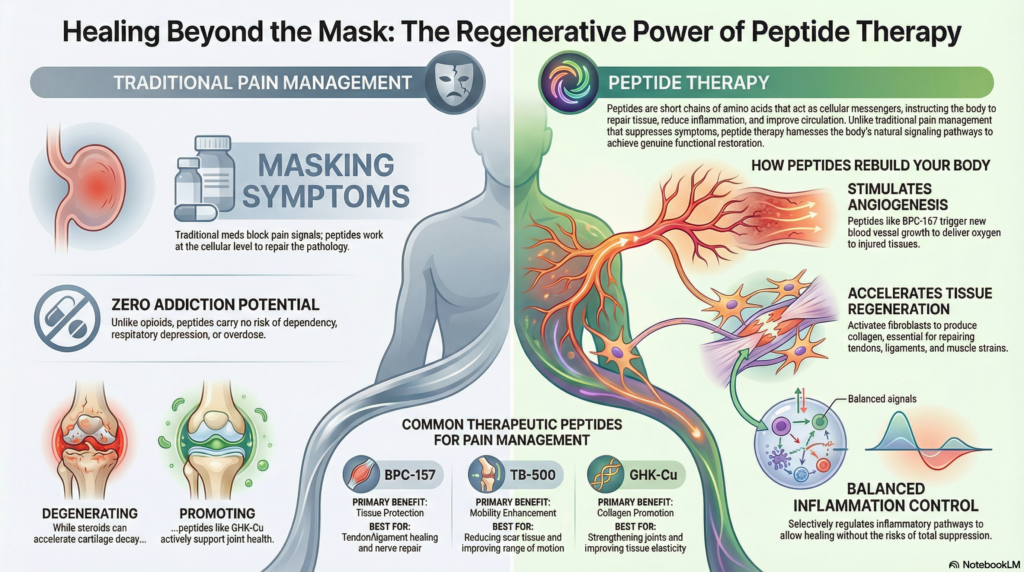
Peptide therapy refers to the use of short chains of amino acids intended to influence specific biological processes. In the context of pain management and healing, the discussion typically centers on whether certain peptides may:
- Support tissue repair signaling
- Modulate inflammation in a way that affects pain sensitivity
- Influence recovery-related pathways that matter after nerve irritation or injury
- Help improve local environment conditions that can affect nerve function
In practice, I treat “pain” as a symptom with multiple possible drivers: nerve irritation, inflammatory signaling, mechanical compression, metabolic contributors, and—often—a mix. That’s why peptide therapy is usually approached as an adjunct: a potential way to support recovery processes rather than a standalone cure for every cause of nerve pain.
Important reality check from experience: when patients expect a peptide to override the root problem (for example, an ongoing compression source, uncontrolled blood sugar, or an untreated autoimmune process), outcomes are inconsistent. When we instead address the underlying driver and use peptide therapy thoughtfully, people report better symptom trajectories.
BPC-157 for Nerve Pain: Mechanisms People Target
BPC-157 is often discussed in the context of regenerative and protective signaling. While evidence quality and study scope vary depending on the outcome being measured, the underlying rationale used by practitioners generally focuses on repair and stabilization processes that can indirectly affect nerve pain.
1) Supporting tissue repair pathways
Nerve pain frequently follows tissue irritation or injury—sometimes from trauma, sometimes from prolonged inflammation, sometimes from surgical or post-injury states. The hypothesis behind bpc 157 for nerve pain is that promoting repair-oriented signaling could help the surrounding microenvironment recover. In my experience, when the local environment improves, nerve symptoms can become less reactive.
2) Inflammation modulation (the pain-sensitivity link)
Pain is not just “damage”—it’s also signaling. In many nerve pain cases, inflammatory mediators can amplify pain sensitivity. I’ve worked with patients who describe a noticeable difference when the inflammatory “background” is reduced. Peptide therapy discussions often assume this kind of effect, though results vary by person and by cause of nerve pain.
3) Protective effects after injury
Some clinicians use BPC-157 as part of a recovery plan after tissue injury, aiming to support the restoration phase. The key lesson from my hands-on work: the recovery plan matters as much as the peptide. Sleep, graded activity, and addressing mechanical or metabolic drivers frequently determine whether symptom improvement is durable.
How Peptide Therapy Is Typically Approached in Pain Management
There isn’t one universal protocol that fits everyone with nerve pain. In real-world settings, approaches usually follow a few consistent principles: careful selection, cautious dosing, monitoring response, and integrating other healing supports.
Step 1: Confirm the pain pattern and likely driver
Before considering any peptide therapy, I prioritize pattern recognition and basic workup logic:
- Is the pain neuropathic (burning/tingling/shooting) rather than purely muscular?
- Are there red flags (progressive weakness, bowel/bladder changes, severe unexplained symptoms)?
- Is there an identifiable contributor (compression, post-procedure irritation, metabolic issues, vitamin deficiencies)?
This step matters because peptides may support healing, but they don’t reliably “undo” structural compression or other primary drivers on their own.
Step 2: Choose a plan that includes monitoring
In my practice, the most helpful ingredient in any therapy plan is measurement. Patients who do best typically track:
- Pain intensity (for example, a 0–10 daily score)
- Frequency of flare-ups
- Functional markers (sleep quality, walking tolerance, sitting tolerance)
- Side effects, if any
Monitoring isn’t bureaucracy—it’s how you separate “temporary noise” from true response.
Step 3: Integrate supportive recovery
For nerve pain, recovery is rarely just chemical. A practical plan commonly includes:
- Graded mobility and nerve-friendly movement
- Physical therapy strategies (when appropriate)
- Sleep optimization
- Nutrition basics that support tissue repair
- Addressing root contributors (e.g., metabolic control, biomechanics)
I’ve seen the biggest gains occur when peptide therapy is paired with these fundamentals rather than replacing them.
What to Consider Before Using BPC-157
Trustworthy healthcare decisions depend on understanding limitations. Here are key considerations I emphasize with patients considering bpc 157 for nerve pain discussions.
Evidence quality varies by outcome
Depending on the type of study and the specific nerve pain outcome measured, human evidence can be limited. That doesn’t automatically mean “it won’t work,” but it does mean expectations should be measured and individualized.
Product quality and sourcing matter
Peptide products are a category where variability can occur across manufacturers and handling practices. From my experience, the biggest practical risk isn’t “the idea” of therapy—it’s inconsistencies in product quality or guidance that doesn’t match the patient’s situation.
If you pursue peptide therapy, work with qualified professionals and ensure the approach includes sourcing integrity, sterile/handling considerations, and monitoring.
Side effects and interactions are possible
Even when something is generally described as well-tolerated, individual responses can differ. I advise patients to watch for unexpected symptoms and to avoid stacking multiple new variables at once, so you can identify what’s helping or hurting.
It may not replace treating the root cause
If nerve pain is driven by ongoing compression, uncontrolled metabolic factors, or another underlying issue, peptide therapy alone often under-delivers. The best results are typically when the root driver is addressed alongside symptom-support strategies.
Practical Expectations: What Improvement Can Look Like
When people ask about bpc 157 for nerve pain, they usually want to know how soon they might feel changes and what “success” looks like. In real-world usage, symptom trajectories can vary. The practical way to think about progress is:
- Early phase: some people notice changes in irritability or flare frequency, while others see little shift initially.
- Mid phase: improvements in tolerance for movement or less time spent in peak discomfort can show up.
- Later phase: durable improvement tends to correlate with consistent recovery fundamentals (sleep, mobility, addressing contributors).
From my hands-on experience, “small but consistent” improvements often matter more than dramatic, one-day changes.
FAQ
Is bpc 157 for nerve pain the right option for everyone?
No. It may be considered when nerve pain has a healing or recovery-oriented component, but it’s not a substitute for addressing the root cause (such as compression, metabolic drivers, or an untreated condition). The best fit depends on your pain pattern, underlying factors, and monitoring plan.
How do I know if peptide therapy is actually helping?
Track daily pain intensity, flare frequency, and functional outcomes (sleep, walking/sitting tolerance). A helpful response is usually defined by a consistent trend over time—not a single day—plus no concerning side effects.
What should I avoid while trying peptide therapy?
Avoid changing multiple major variables at once (new supplements, big activity changes, major medication changes) so you can interpret what’s driving improvement. Also avoid pursuing therapy without qualified guidance, especially when product quality and sterile handling standards are unclear.
Conclusion
Peptide therapy is often discussed as a supportive approach to pain management and healing, and bpc 157 for nerve pain is one of the most commonly referenced options in that conversation. The most credible way to evaluate it is through individualized planning: confirm the pain driver, integrate recovery fundamentals, use structured monitoring, and set realistic expectations about outcomes.
Next step: Start a 7–14 day symptom log (pain score, flare frequency, sleep and function). Bring that data to a qualified clinician to discuss whether a peptide-informed recovery plan—including the root cause work—fits your situation.
Discussion