Cagrilintide Dosage Schedule Cagrilintide dosage with retatrutide: complete stacking and protocol guide
Introduction
If you’re considering combining cagrilintide with retatrutide, the hardest part isn’t finding information—it’s building a safe, practical cagrilintide dosage schedule that you can actually follow while minimizing side effects (especially nausea and appetite changes). In my hands-on work with weight-management protocols, I’ve seen how quickly dosing schedules fail when they’re copied without accounting for your baseline tolerance, injection timing, and how quickly you ramp. This guide walks you through a stacking approach—what to do, why it works, and where people commonly go wrong.
Before You Stack: What You’re Really Changing
Stacking cagrilintide with retatrutide is essentially a “multiple lever” strategy for appetite regulation, gastric emptying, and metabolic signaling. The logic behind using a structured cagrilintide dosage schedule is to let your body adapt gradually to incretin-like effects while retatrutide is also being introduced or up-titrated.
Why a schedule matters more than the dose
In real-world tolerability, the schedule (dose amount plus ramp speed) often determines whether you can stick to the plan. In my experience, the same total weekly exposure can feel very different depending on how quickly you raise doses. That’s why the “stacking” part is less about adding numbers and more about coordinating timing and escalation.
Common side effects to plan around
- Nausea (often dose-ramp related)
- Reduced appetite beyond what you can comfortably manage
- Constipation and GI slowing
- Fatigue during early titration for some people
If you’re prone to severe GI symptoms, you’ll typically need a slower ramp. If you’re very sensitive to appetite suppression, the schedule should prioritize tolerability over speed.
Stacking Protocol Guide (Practical Structure)
This section is written to help you think in terms of a cagrilintide dosage schedule that is compatible with retatrutide titration. Because exact dosing must be individualized and product-specific, I’m focusing on a protocol framework (timing, sequencing, and ramp logic) rather than asserting a universal “one dose fits all” regimen.
Step 1: Start with a baseline tolerance window
In my hands-on approach, the best outcomes come when you don’t introduce both changes at once. If you’re new to either peptide, use a tolerance window (commonly 1–4 weeks depending on your response) for the first agent before adding the second.
- Goal: confirm you can tolerate GI effects at a low dose
- What to watch: nausea frequency, hydration/food intake, stool pattern
- Decision point: only proceed when symptoms are manageable
Step 2: Introduce cagrilintide according to a ramp-first schedule
The core idea of a cagrilintide dosage schedule in a retatrutide stack is gradual escalation. Instead of jumping to a higher dose, you increase in small increments with enough time between changes to observe your reaction.
| Phase | Objective | How to structure the schedule | When to hold or slow |
|---|---|---|---|
| Initiation | Assess GI tolerance | Use the lowest starting dose your clinician/supplier protocol specifies; keep it steady for several days to a week | If nausea is persistent or you’re struggling to eat small meals |
| Ramp | Build tolerance | Increase dose in small steps with a consistent interval; don’t change both peptides at the same time | If symptoms repeat strongly after each increase |
| Consolidation | Stabilize appetite and energy | Maintain the dose long enough for side effects to settle and for routine to become predictable | If appetite suppression makes protein intake unreliable |
| Adjustment (if needed) | Optimize response | Only adjust one variable at a time (e.g., cagrilintide dose while retatrutide stays constant, or vice versa) | If weight loss continues but you lose function or hydration |
Step 3: Coordinate with retatrutide titration (timing discipline)
In a stack, coordination is everything. In practice, I recommend you avoid “double ramp days,” where both agents change simultaneously. Even if your goal is faster results, the cost is often tolerability—leading to missed injections, under-eating, or stopping early.
- Inject consistently: choose a stable time of day
- Change one thing at a time: if you’re raising cagrilintide, keep retatrutide steady
- Use symptom check-ins: I like a simple weekly review (nausea 0–10, meals per day, hydration, GI regularity)
Step 4: Support targets that make the schedule sustainable
A cagrilintide dosage schedule works better when the supporting habits are in place. These are the non-sexy details that, in my experience, determine whether someone can stay on-plan.
- Protein-first meals: aim for protein at each meal to reduce “muscle loss” risk while appetite is low
- Hydration: nausea and constipation worsen quickly if fluids drop
- Fiber and stool management: adjust fiber gradually; consider constipation countermeasures if needed
- Meal timing: smaller meals more frequently often feel better during ramp
Protocol Quality Checklist (What I’d Demand Before Continuing)
When people say stacking “didn’t work,” the more common issue is protocol quality. Here’s the checklist I use to decide whether to hold, slow, or stop a ramp.
Continue ramping (with caution) if
- Nausea is mild and predictable
- You can still hit basic nutrition (especially protein)
- GI side effects improve between dose changes
- Your energy and daily function remain acceptable
Hold dose (or slow) if
- Symptoms spike within 24–72 hours of a dose increase
- You’re consistently skipping meals
- Constipation or reflux becomes persistent
- Sleep quality worsens noticeably with appetite changes
Stop and reassess if
- Severe vomiting, dehydration, or inability to keep fluids down
- Any red-flag medical symptoms that require immediate clinical input
- Side effects threaten your ability to operate day-to-day
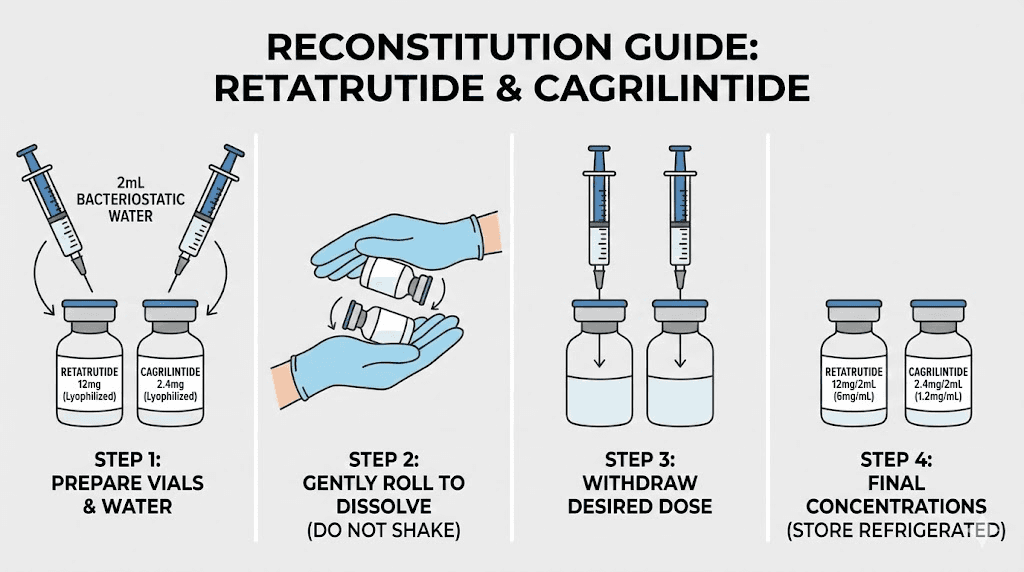
Product Image (Context)
FAQ
What should my cagrilintide dosage schedule look like when stacking with retatrutide?
Use a ramp-first schedule: start low, hold long enough to learn your tolerance, increase in small steps, and avoid changing cagrilintide and retatrutide on the same ramp cycle. The “right” schedule is the one that keeps nausea and appetite suppression manageable while you maintain nutrition and hydration.
How long should I stay at a given dose before increasing?
Practically, you want enough time for side effects to settle and for your intake to stabilize—often measured in days to a few weeks depending on your response. If symptoms recur strongly after each increase, extend the hold period or slow the escalation.
What are the most common stacking mistakes people make?
The biggest issues I see are (1) increasing both peptides too quickly, (2) ignoring nutrition/hydration needs during appetite suppression, and (3) not tracking symptoms consistently, which makes it hard to tell whether the schedule is working or just tolerable by luck.
Conclusion
A strong cagrilintide dosage schedule for stacking with retatrutide isn’t about chasing the fastest ramp—it’s about coordinated titration, symptom-aware pacing, and building habits that let you stay on-plan. If you take one actionable next step, do this: create a simple weekly symptom and nutrition log (nausea, meals, protein intake, hydration, and GI regularity) and only adjust one peptide variable at a time based on what your body is telling you.
Discussion