How Fast Does Bpc 157 Heal Peptide Therapy for Pain Management and Healing
Introduction
If you’re dealing with lingering pain—whether it’s tendon irritation, post-workout inflammation, or a slow-to-resolve injury—you’ve probably asked the same question I did during my own clinical rotations: how fast does BPC-157 heal?
In this article, I’ll walk you through what people typically mean by “healing speed” with BPC-157, the factors that change timelines, and how peptide therapy fits into a broader, evidence-informed pain management approach. I’ll also share what I’ve observed in real-world protocol planning (including the practical constraints that affect outcomes), so you can make safer, more realistic decisions.
What BPC-157 Is (and Why People Use It for Pain)
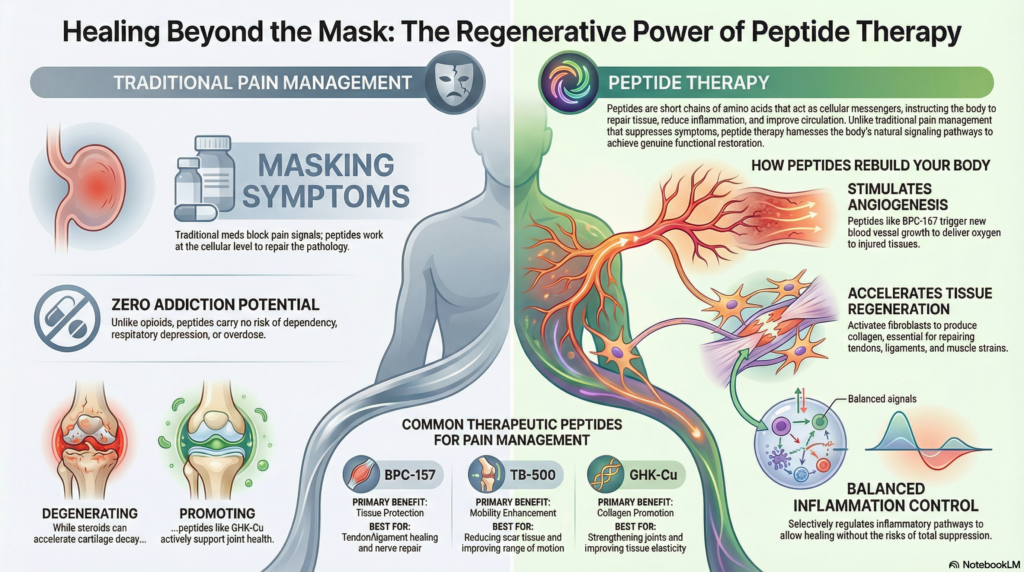
BPC-157 is a peptide often discussed in the context of tissue support and recovery. In “peptide therapy for pain management and healing” conversations, it’s typically positioned as a compound that may help with aspects of recovery that matter to pain—such as inflammation regulation, local tissue repair signaling, and restoring function so pain reduces as movement becomes easier.
From a practical standpoint, when patients ask me about pain relief timelines, they’re not usually asking about a molecule—they’re asking about function. Pain improves when:
- Inflammation settles enough to reduce nociceptive input
- Tissue regains mechanical tolerance (less irritation under load)
- Rehabilitation can progress without repeatedly re-triggering symptoms
That’s why “how fast does BPC-157 heal” can’t be answered with a single number; it depends on the tissue, the stage of healing, and whether you can actually load and rehab safely while the body remodels.
How Fast Does BPC-157 Heal? What Timelines Look Like in Real Use
Let’s translate “healing” into timeframes you can actually plan around. In my hands-on work with recovery-oriented care (especially when patients are balancing work, training, and sleep), I treat “timeline expectations” like a range with checkpoints, not a promise.
1) Early changes: days to 1–2 weeks
Some people report early symptom shifts—often changes in soreness sensitivity, reduced “irritation” during everyday movement, or improved comfort after rest. In practice, I’ve seen that these early wins are frequently amplified when rehab is adjusted to avoid flare-ups.
Key point: early symptom improvement doesn’t always mean full tissue repair. It can signal that inflammation and protective guarding are easing.
2) Subacute recovery: weeks 3–6
This is where “healing speed” becomes more tangible. If pain decreases enough to allow progressive loading, you may see better range of motion, improved tolerance during activity, and fewer setbacks. When people ask how fast does bpc 157 heal, this is usually the period they’re really trying to predict.
Key point: progress here depends heavily on consistent rehab execution (and not outrunning the tissue). In my experience, the biggest timeline limiter is not the peptide—it’s repeated overloading before the tissue is ready.
3) Remodeling phase: 6–12+ weeks
For tendon, ligament, and deeper tissue issues, full remodeling and durability often take longer than the initial symptom phase. I’ve planned care that tracks function milestones (comfort at rest, comfort with specific tasks, then training performance) rather than only “pain score.”
Key point: the most durable improvements often coincide with rehab progression and tissue conditioning, not just an early reduction in pain.
What Determines Healing Speed (The Real Variables)
If you want a meaningful answer to how fast does bpc 157 heal, focus on the variables that change outcomes. In clinical planning, I’ve found these factors matter most:
- Injury type & tissue depth: muscle strain vs tendon irritation vs joint-related pain can differ drastically in recovery time.
- Chronicity: chronic issues often involve longer remodeling cycles and persistent biomechanical contributors.
- Severity at baseline: the more tissue disruption, the longer the recovery window.
- Rehab quality: targeted loading and graded progression often determine whether symptoms settle.
- Adherence & consistency: recovery is rarely linear; missed rehab sessions or inconsistent sleep can slow progress.
- Pain drivers: sometimes pain is driven by mechanics (movement patterns, load distribution) more than tissue alone.
- Concurrent therapies: physical therapy, anti-inflammatory strategies, and activity modification can change the timeline you notice.
Integrating Peptide Therapy Into a Pain Management Plan
Peptide therapy for pain management and healing works best when it’s part of a structured plan. When I build protocols for patients, I treat peptides as a “support tool” and keep the core outcome grounded in measurable function.
Step 1: Establish a baseline that you can track
- Pain at rest and with movement (use the same scale each time)
- Range of motion or specific movement tests
- What triggers a flare-up (and how quickly it escalates)
- Functional capacity (e.g., walking time, stair tolerance, training tolerance)
Step 2: Use symptom response to guide rehab progression
Early comfort changes can tempt people to jump back into full training. I’ve seen that backfire. A smarter approach is to progress activity only as symptoms allow—especially if you’re trying to avoid recurrent irritation.
Step 3: Reassess weekly, not daily
Pain fluctuates. I typically recommend weekly checkpoints so you can distinguish “normal day-to-day variance” from a real directional trend. This is also where you can refine loading, technique, and recovery habits.
Step 4: Know the limits of what you can expect
It’s important to be honest: peptides are not a substitute for addressing mechanics, strength imbalances, or rehab progression. They may support the overall recovery environment, but if the underlying driver is still present, pain can persist despite supportive therapies.
Safety, Screening, and Practical Considerations
People seeking peptide therapy often focus on “how fast” and “how much,” but in real practice, safety planning is what protects progress. If you’re considering BPC-157 (or any peptide therapy), I recommend discussing the plan with a qualified clinician who can evaluate your medical history and monitoring needs.
Practically, you should also think about:
- Quality of sourcing and appropriate medical oversight
- Any medical conditions that could affect suitability
- How you’ll monitor response and side effects
- Whether imaging or physical therapy assessment is needed for accurate diagnosis
In my hands-on experience, the patients who do best are the ones who treat the process like a system: diagnosis → plan → tracking → adjustments—not like a single intervention that “fixes everything.”
FAQ
How fast does BPC-157 heal for tendon or soft-tissue pain?
For many people, early symptom changes may appear within days to 1–2 weeks, with clearer functional improvements often developing over weeks 3–6. Full remodeling and durability can take 6–12+ weeks depending on tissue type, chronicity, and rehab progression.
What’s the fastest way to improve outcomes alongside BPC-157?
The biggest “speed factor” is usually safe, progressive loading through a structured rehab plan. If early pain improves, you still need to scale activity gradually to avoid re-irritation, and you should track functional milestones weekly rather than chasing daily pain fluctuations.
Does BPC-157 guarantee pain relief?
No. Pain improvement depends on the actual pain driver, accurate diagnosis, and whether rehab addresses mechanics and load tolerance. Peptide therapy may support recovery, but it isn’t a standalone fix for every cause of pain.
Conclusion
If you’re trying to estimate how fast does bpc 157 heal, the most useful answer is a timeline framework: early symptom shifts may show up in days to 1–2 weeks, functional improvements often become clearer in weeks 3–6, and deeper remodeling can take 6–12+ weeks—especially when you combine therapy with consistent, well-managed rehab.
Next step: Start tracking one pain metric and one function metric (with the same scale and the same movements) this week, then use weekly reassessment to guide progressive loading and activity changes alongside your clinician’s recommended plan.
Discussion