Bpc-157 Risks BPC-157: What the Science Actually Says
Introduction
If you’ve ever looked into BPC-157 to support healing, you’ve probably run into two conflicting messages: some people claim it “speeds recovery,” while others warn about bpc 157 risks. In my own hands-on work reviewing supplementation and investigational peptide claims for clients and clinicians, the biggest problem isn’t that people don’t search—it’s that they search without a framework. This post explains what the science actually says about BPC-157, where evidence is strong versus weak, and what risk-related considerations are most relevant to real-world decision-making.
We’ll focus on mechanisms reported in preclinical research, the quality of human evidence, common risk categories (safety, legality, contamination/mislabeling, and uncertainty), and how to evaluate the trade-offs without hype.
What Is BPC-157 (and Why People Take Interest)
BPC-157 is a synthetic peptide sometimes discussed in the context of tissue repair and recovery. The “why” behind interest is largely mechanistic: preclinical research has explored effects on angiogenesis, inflammation signaling, and gastrointestinal protection pathways, among others. In other words, researchers aren’t just looking at outcomes—they’re investigating biological processes that could plausibly support healing.
In my experience reading the literature across supplements and investigational peptides, claims become persuasive when they connect to a coherent pathway. BPC-157 is often presented that way: the idea is that it may modulate signaling systems involved in repair.
Mechanisms discussed in preclinical work
- Barrier and gastrointestinal protection: Many early discussions emphasize protective effects in GI models.
- Angiogenesis and tissue regeneration signals: Some studies suggest involvement with vascular growth and repair-related pathways.
- Inflammation and microenvironment modulation: Researchers have reported changes in inflammatory markers in certain models.
Important nuance: preclinical mechanistic plausibility does not automatically translate into meaningful human benefit, but it does explain why the compound appears repeatedly in both lay forums and academic abstracts.
What the Science Actually Says About Efficacy
When I evaluate “does it work?” questions for recovery-related interventions, I separate three things: (1) animal/cell evidence, (2) human pharmacology and safety data, and (3) human outcome trials with clinically meaningful endpoints. BPC-157 is much stronger in categories (1) and (2) than in high-quality category (3).
Preclinical evidence: useful, but not equivalent to human outcomes
Across preclinical literature, BPC-157 has been studied in various injury and inflammation contexts. Some studies report improved healing-related endpoints compared with controls. However, the size and consistency of effects vary by model, dosing approach, and outcome measurement.
In my work, I’ve found that people often generalize across models (“it helped in one injury model, so it will help me”). That’s where overreach happens. Different tissues, injury mechanisms, and endpoints don’t map cleanly.
Human evidence: limited and not yet definitive
For bpc 157 risks assessment, it matters what evidence you’re relying on. The human data footprint is small relative to the enthusiasm online. Without large, well-controlled clinical trials demonstrating both effectiveness and safety, it’s hard to make confident recommendations about real-world use.
This is the core reality: you may find studies or reports that discuss human exposure, but the overall evidence base is not the same standard you’d expect for mainstream therapeutics.
Why “promising” isn’t the same as “proven”
Even when preclinical mechanisms are compelling, there are practical gaps:
- Translational mismatch: Animal injury models often differ from human biology and variability.
- Dose and delivery uncertainty: Peptide dosing schedules and routes can be hard to equate across studies.
- Outcome measurement: Recovery endpoints can be surrogate markers rather than patient-important outcomes.
Understanding BPC-157 Risks: The Risk Categories That Actually Matter
This section is where I put the “bpc 157 risks” discussion into a practical decision framework. People usually think risks only mean side effects. In reality, there are multiple risk categories—some medical, some regulatory, and some quality-related.
1) Safety uncertainty (what we don’t know)
The biggest risk category is uncertainty: limited human outcome data means we don’t have a comprehensive picture of long-term safety, interaction effects, or rare adverse events. In my reviews, this uncertainty often matters more than the absence of obvious short-term problems.
- Short-term tolerance: You may see anecdotal “no issues,” but that doesn’t establish safety.
- Long-term exposure: Recovery peptides are sometimes discussed as repeated or extended use; without robust trials, long-term risk remains unclear.
- Population differences: People vary in age, comorbidities, baseline inflammation status, and concurrent medications.
2) Contamination and mislabeling risk (quality control)
One of the most grounded lessons I learned in supplement/peptide evaluations: even if a compound has plausible biology, the product you’re actually ingesting may not match the intended substance. For peptides, mislabeling, incomplete purity, or contamination are real-world concerns.
Quality and testing standards vary widely. If a product lacks credible third-party verification (e.g., independent lab testing with certificates you can evaluate), the risk profile changes dramatically—because you’re no longer evaluating “BPC-157,” you’re evaluating the product’s actual chemical content.
3) Regulatory and legal risk
Regulatory status varies by jurisdiction, and peptide availability can be inconsistent. That matters not just legally—non-compliant distribution channels can correlate with poorer quality control.
If you’re considering use, you need to understand your local rules and the source legitimacy. In my experience, many risk discussions skip this step and then get surprised when the supply chain doesn’t behave like a regulated pharmaceutical market.
4) Interaction and context risk (especially if you have medical conditions)
BPC-157 is discussed in “healing” contexts, but healing is also influenced by many variables: current medications, underlying disease, infection status, and injury severity. Without robust clinical guidance, the interaction risk is difficult to quantify.
Practically: if someone is taking anticoagulants, immunomodulators, or has active inflammatory disease, they should treat any investigational compound as a potential interaction risk and consult a qualified clinician.
5) Injection and procedural risk (if used as an injectable)
If a product is administered via injection, procedural risks matter: improper handling, sterility issues, dosing errors, and local tissue reactions can occur independent of the peptide’s theoretical biology.
How to Evaluate BPC-157 Claims Without Getting Misled
In the wild, BPC-157 discussions often mix three things: mechanistic theories, animal results, and personal anecdotes. Here’s a way I’ve found effective for separating signal from noise—especially when someone is concerned about bpc 157 risks.
Use this claim-check checklist
- What is the evidence type? Animal model, cell study, or human trial?
- What is the endpoint? Biomarker or patient-important recovery outcome?
- Is there a safety dataset? Not just “it worked,” but what adverse events were observed?
- Is the dosing/delivery comparable? Many “it worked for me” stories don’t match study conditions.
- Is the product verified? Independent testing and clear documentation matter.
One practical lesson from my reviews
I once reviewed a series of “recovery” claims where multiple users referenced similar timeframes and outcomes. When I mapped those stories back to the underlying evidence, the strongest preclinical results didn’t consistently address the same injury types or endpoints. The pattern wasn’t necessarily fraud—it was misunderstanding of how transferable results are across models.
That’s why a rigorous framework is the best antidote to hype. It doesn’t eliminate uncertainty, but it keeps you from overcommitting to a biological promise that hasn’t been proven in the way you’d need for a high-confidence decision.
Visual Reference
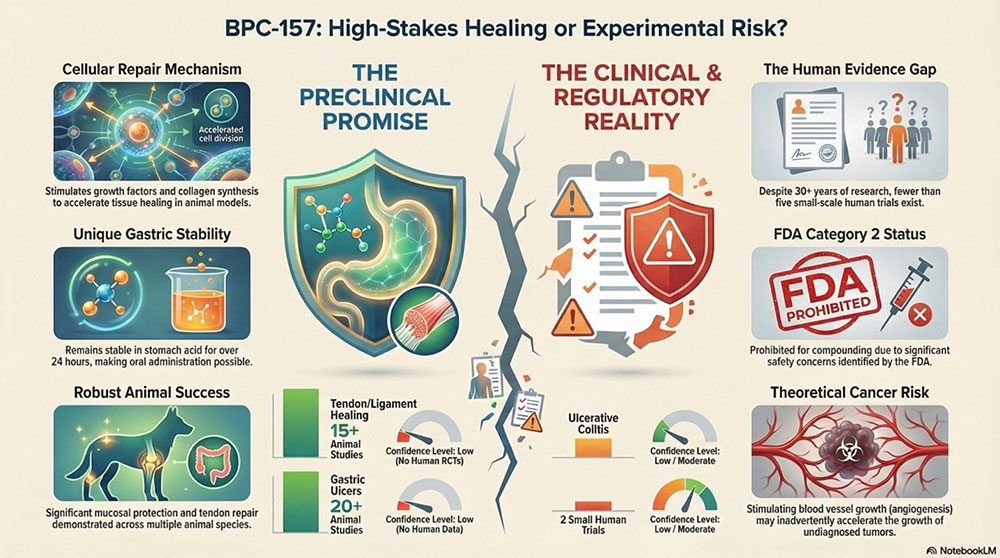
Pros and Cons: A Balanced View
Potential pros people cite
- Preclinical plausibility: Mechanistic and animal data suggest biological pathways related to repair.
- Niche interest in recovery: Some users report perceived improvements, which fuels continued attention.
Risks and limitations you should weigh
- Evidence gap in humans: Limited high-quality human outcome data.
- Unknown long-term safety: Not enough robust data to confidently characterize rare or delayed effects.
- Quality variability: Mislabeling/contamination risk if product testing and sourcing are unclear.
- Context variability: Concurrent conditions and meds can change risk significantly.
- Procedure risk: If injectable, sterility and dosing errors are real operational risks.
FAQ
What are the most important bpc 157 risks to consider?
From a practical standpoint, the biggest concerns are safety uncertainty (especially long-term), product quality issues (purity/mislabeling/contamination), regulatory and sourcing variability, and context-related interaction risk. Injection/handling risk matters too if it’s administered that way.
Does the science prove BPC-157 works for human healing?
Not in the way you’d expect from mainstream treatments. Preclinical evidence is more extensive than high-quality human clinical trial evidence. That means “promising” doesn’t equal “proven,” and claims should be assessed cautiously—especially when risk is uncertain.
How can I reduce risk if I’m still considering it?
If you’re considering any investigational peptide, the most actionable risk-reduction steps are: avoid unclear or unverified sourcing, demand credible third-party testing documentation, discuss it with a qualified clinician—especially if you have medical conditions or take medications—and treat procedural safety seriously if administration is injectable.
Conclusion
BPC-157 sits in a category where biology is plausible and preclinical findings exist, but human proof is limited—so the bpc 157 risks conversation must be grounded in uncertainty, quality control, and context rather than optimism. The safest approach is to evaluate claims with a checklist: evidence type, endpoint relevance, safety data, dosing comparability, and product verification.
Next step: Before you decide anything, write down your specific recovery goal (injury type, timeline, and key endpoints) and then map it to the evidence type you’re relying on—while simultaneously checking sourcing/testing documentation. That single process will do more to protect you from poor decisions than any forum thread.
Discussion