Bpc 157 Adverse Effects BPC-157: Tendon Repair and More
Introduction: why “BPC-157 for tendon repair” deserves a cautious, evidence-based look
If you’ve ever dealt with tendon pain that lingered for months—thick tendon swelling, limited range of motion, and the frustrating cycle of rehab that stalls—you already know the emotional cost of slow healing. In recent years, bpc 157 adverse effects has become one of the first questions people ask before considering BPC-157. That’s exactly the right instinct.
In this article, I’ll walk you through what BPC-157 is commonly used for (especially tendon repair), what the real-world decision process looks like, and how to think about potential bpc 157 adverse effects without hype—so you can make safer, smarter calls with your clinician and rehab plan.
What BPC-157 is—and why tendon repair is a common focus
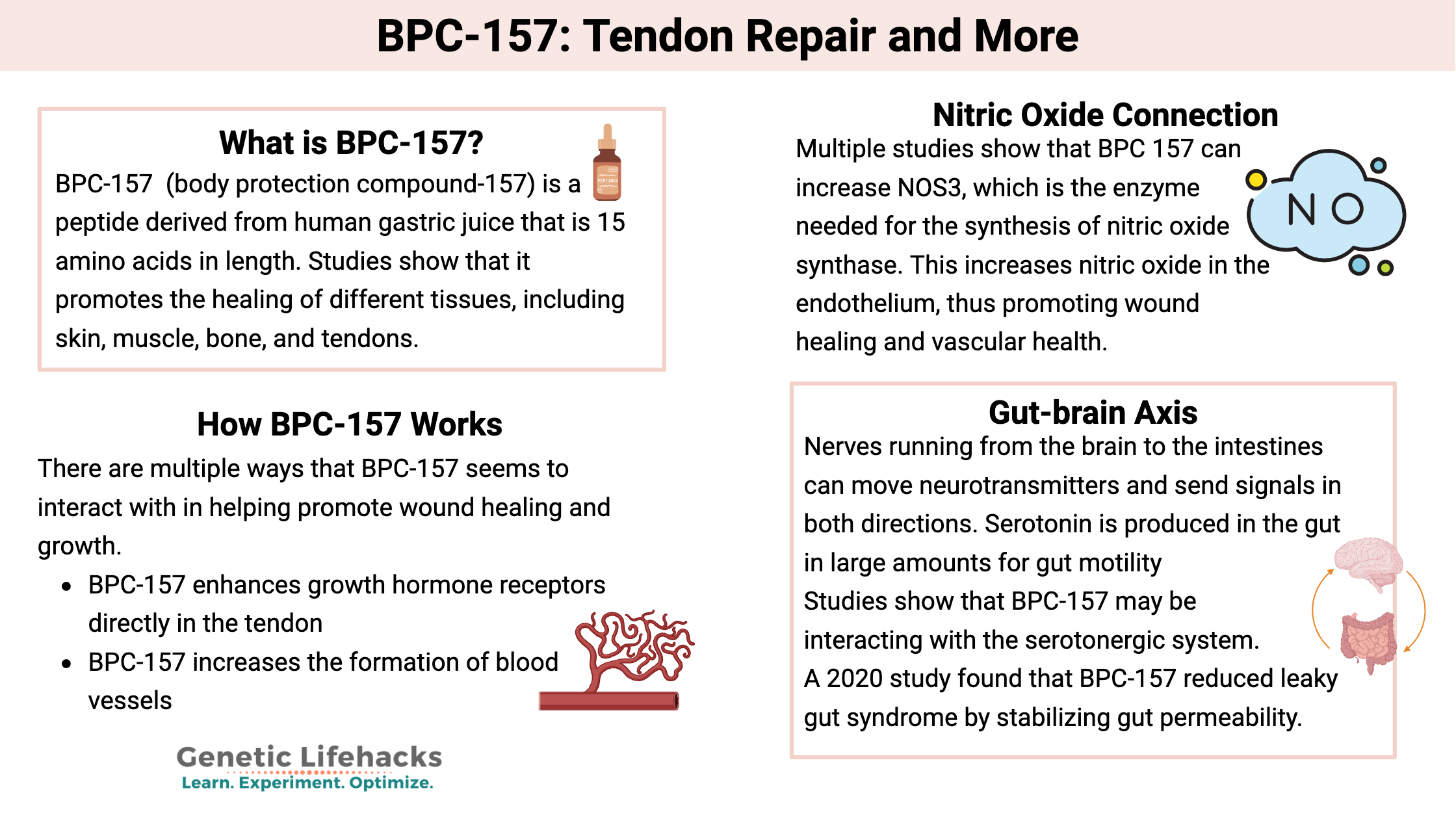
BPC-157 is a peptide that’s discussed in alternative and research-leaning communities for tissue support, with a strong emphasis on healing outcomes in injuries such as tendon strains and tendinopathies. The reason tendon repair is so frequently mentioned is that tendons are notoriously slow to recover compared with many other tissues, partly due to limited blood supply and the way collagen remodeling responds to load over time.
In hands-on rehab work with injured athletes and active clients, I’ve seen two patterns that matter when people consider any “healing support” supplement or peptide:
- Stalled remodeling: pain improves, but the tendon doesn’t regain capacity quickly enough to tolerate progressive loading.
- Load-response mismatch: people either overload too early (re-aggravation) or offload too long (deconditioning of tendon capacity).
BPC-157 is often discussed as a way to support the biology around healing and remodeling. However, it’s crucial to separate “mechanism-based hope” from clinical certainty. When I evaluate options with patients, I treat peptides like BPC-157 as adjuncts to a structured plan—not replacements for progressive tendon loading, tendon-friendly mobility, and clinician-guided care.
How tendon repair typically works in real life (and where BPC-157 fits, if at all)
Tendon recovery is usually a staged process: inflammation/irritability settles, then tendon cells and collagen alignment adapt, and finally the tendon builds tensile capacity through progressive loading. This is why the “best” approach for tendon repair rarely looks like one intervention—it looks like a timeline.
My practical rehab lens: biology plus loading
In my hands-on work, I’ve found that success depends on matching intervention intensity to tendon irritability. For example, when a client’s tendon is highly reactive, we prioritize pain-calming strategies and isometrics first. As irritability drops, we move to structured strength and eccentric/concentric loading progressions.
If someone adds a peptide or supplement during this period, it should never disrupt the basics. The load plan still needs to be coherent and measurable (symptoms during loading, next-day response, and functional milestones).
Where “BPC-157 for tendon repair” conversations often help
Even when the evidence base is limited, the discussion can still be useful if it pushes people to plan better:
- track symptoms consistently (pain scale, stiffness, function)
- advance load gradually with clear criteria
- avoid “try everything at once” so you can tell what’s working
BPC-157 adverse effects: what to consider before you decide
Let’s get straight to the key concern: bpc 157 adverse effects. Because BPC-157 is not broadly approved as a standard medical treatment in many regions, high-quality, large-scale safety data can be limited. That doesn’t mean “it’s unsafe,” but it does mean your risk thinking should be conservative.
From an evidence and safety-management perspective, potential adverse effects that people discuss fall into a few broad categories. I’m not claiming these will happen to everyone—rather, these are the types of concerns you should actively screen for and discuss with a clinician.
1) Unknown long-term safety
One of the biggest trust issues with peptides outside mainstream approval pathways is uncertainty around long-term outcomes. In my experience, people underestimate how important “time horizon” is: a short trial can feel fine, but you may not know delayed effects, especially if dosing and purity vary.
2) Product quality and contamination risk
In real-world scenarios, adverse effects are sometimes not from the molecule itself, but from inconsistencies in:
- purity
- mislabeling
- contaminants
- storage instability
This is why I strongly emphasize sourcing diligence and medical oversight when people ask about peptides. Even if you “tolerate” a product, the quality variables can still create safety and effectiveness problems.
3) Individual intolerance or unexpected symptoms
Some people may experience reactions that are best treated as “tolerance signals,” such as gastrointestinal discomfort, headaches, changes in sleep, or general malaise. If you notice symptoms after starting, the correct workflow is to stop and get medical advice—don’t push through while also advancing rehab load.
4) Interactions with your rehab and training plan
This isn’t a “side effect” in the traditional sense, but it matters: if you feel better faster, you may be tempted to progress too quickly. That can worsen the injury even if the peptide itself is tolerated.
In my casework, the most common “harmful outcome” wasn’t a dramatic medical reaction—it was a rehab timeline break caused by symptom misinterpretation. So if you try any adjunct, keep the load progression conservative and objective.
What I recommend asking a clinician (so you get usable answers)
- “What safety concerns apply to my medical history and current meds?”
- “Are there conditions where a peptide adjunct would be risky for me?”
- “What monitoring would you want if I start anything new?”
- “How should this affect my rehab progression criteria?”
Decision checklist: when BPC-157 conversations are reasonable—and when they aren’t
To keep this practical, here’s how I’d structure a decision in a real clinic-style workflow. It’s not “yes/no for everyone,” but a checklist that reduces reckless experimentation.
More reasonable when you have…
- a clear diagnosis (or at least a clinician-reviewed working diagnosis) for the tendon issue
- a structured rehab plan with measurable progress markers
- medical oversight and a plan for what to do if symptoms change
- high-quality, verifiable sourcing (as much as is realistically possible)
Red flags and better alternatives when you have…
- unexplained tendon rupture risk or severe imaging findings without a medical plan
- multiple unresolved health conditions that complicate risk assessment
- a “stack everything” approach that makes it impossible to attribute outcomes
- no monitoring plan for symptoms, training load, or medication interactions
Alternatives that often move tendon recovery forward (without betting on peptide certainty)
Even if you’re curious about BPC-157, don’t ignore what reliably improves tendon outcomes for many people. In my experience, tendon repair is more predictable when you focus on proven levers first.
- Progressive loading: isometrics, then tendon-strengthening with planned volume and intensity increases.
- Load management: reduce painful aggravation long enough to restore tolerance, then reintroduce gradually.
- Physical therapy techniques: mobility work, mechanics, and retraining (especially if the tendon issue is tied to technique).
- Sleep and nutrition: tissue remodeling needs consistent recovery capacity.
If your goal is true functional return—running, lifting, jumping—these foundations do the heavy lifting. Any adjunct should support that foundation, not replace it.
FAQ
What are the most important bpc 157 adverse effects to watch for?
The most important categories to watch are unexpected symptoms after starting (how your body tolerates it), and issues related to product quality (purity/mislabeled or contaminated batches). Because long-term safety data is limited, monitoring and clinician guidance matter.
Is BPC-157 only for tendon repair?
It’s commonly discussed for tendon and tissue-healing contexts, but people also bring it up for other conditions. In practice, the safest approach is to treat any peptide discussion as a limited-evidence adjunct and rely on a clinician-guided diagnosis plus a structured rehab plan.
Should I change my rehab plan if I’m using BPC-157?
You should not “let symptoms drive progress” in a vague way. Keep rehab criteria objective: pain response during loading, next-day soreness, range of motion, and functional milestones. If symptoms worsen or new adverse effects appear, stop and consult a clinician.
Conclusion: tendon repair is a system—handle bpc 157 adverse effects with the same discipline
BPC-157 is often discussed for tendon repair, but the question of bpc 157 adverse effects is a legitimate safety filter. The most reliable path I’ve seen in real tendon cases is to treat any peptide as an optional adjunct—not the core of the plan—and to keep your rehab strategy structured, measurable, and clinician-aligned.
Next step: write down your tendon diagnosis (or best working diagnosis), your current rehab timeline, and your top 3 objective progress metrics. Then bring that to a clinician and ask how any interest in BPC-157 (and its potential adverse effects, including tolerance and quality concerns) should affect your loading progression.
Discussion