Is Bpc 157 Better Than Tb 500 BPC-157 vs TB-500: Complete Comparison (2026)
Introduction: Why the “BPC-157 vs TB-500” question won’t go away
If you’ve ever been sidelined by a stubborn soft-tissue injury—tendon irritation, slow-to-heal muscle strains, joint flares—you’ve probably searched the same thing I did the first time: “is bpc 157 better than tb 500”. It’s an understandable question, but the honest answer is less about a single winner and more about matching the right peptide approach to the specific injury biology, your dosing tolerance, and your ability to run a structured rehab plan.
In this hands-on comparison for 2026, I’ll break down what BPC-157 and TB-500 are commonly used for, where each one tends to fit, what practical decision factors matter (beyond marketing claims), and how to think about outcomes realistically—so you can make a plan you can actually execute.
Quick context: what these compounds are (and what people use them for)
BPC-157 and TB-500 are peptide products that are often discussed in the context of injury recovery, particularly for soft-tissue healing. In real-world conversations (clinics, sports rehab groups, and supplement procurement channels), people most frequently look at them for scenarios like:
- Delayed tendon healing or irritation that won’t fully settle
- Muscle strain recovery that feels “stuck” past the expected timeline
- Joint discomfort tied to connective tissue stress
- Scar or adhesion concerns after tissue injury (often discussed, with mixed evidence)
One key point I learned the hard way: you can’t evaluate BPC-157 vs TB-500 purely by the peptide name. The rehab protocol, the stage of healing (acute inflammation vs remodeling), loading strategy, and adherence to a progressive plan can have a bigger impact on whether you feel improvement.
Core comparison: BPC-157 vs TB-500 across the factors that actually drive outcomes
Below is how I’d compare them when someone is trying to decide “is bpc 157 better than tb 500” for a specific situation. I’m focusing on decision-relevant factors people run into in practice.
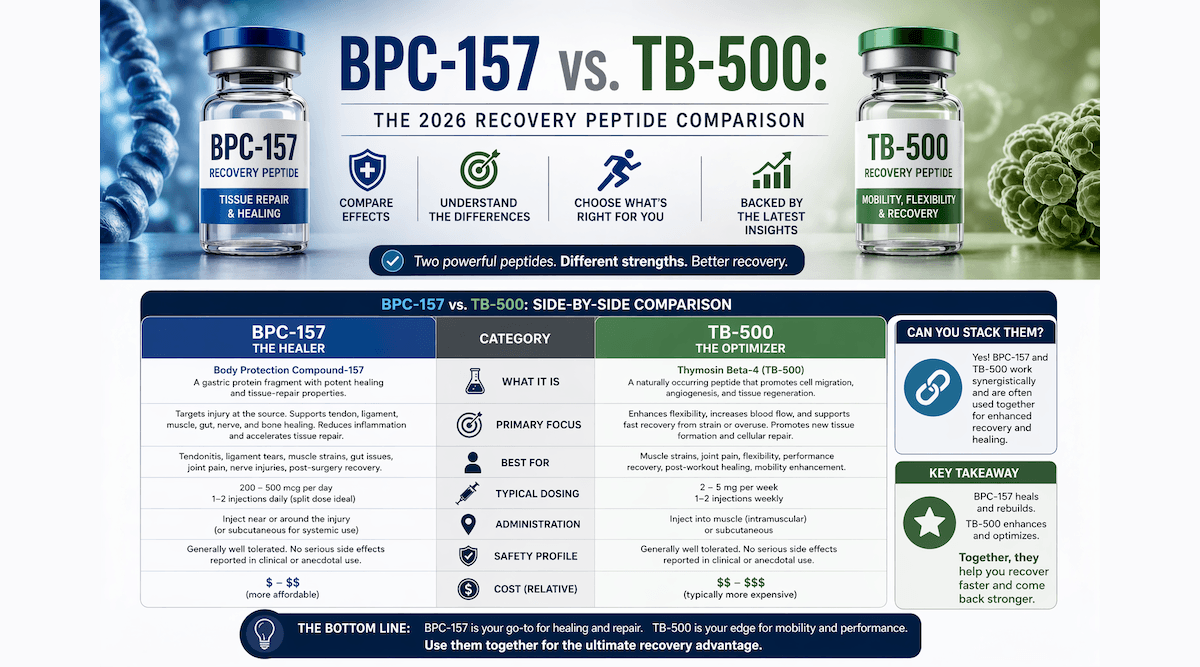
| Factor | BPC-157 (common discussion) | TB-500 (common discussion) | How I’d use this to decide |
|---|---|---|---|
| Primary “reason people try it” | Often used with the goal of supporting recovery and tissue repair processes | Often used with the goal of supporting repair/turnover signaling in connective tissue | Pick based on the tissue problem you’re targeting and the rehab stage—not the hype |
| Typical user profile | People with soft-tissue injuries who want a structured recovery window | People who believe they benefit from a connectivity/repair-focused approach | If your rehab is already solid, peptide choice may matter less than consistency |
| How outcomes are usually evaluated | Symptom reduction + improved tolerance to loading over time | Improved healing trajectory and perceived resilience during training | Use measurable rehab milestones (range of motion, pain-free load, return-to-activity) |
| Practical trial design | Often trialed with close rehab tracking and staged reloading | Often trialed similarly, with emphasis on connective tissue tolerance | Run one variable at a time if you can—otherwise you won’t learn anything |
| Limitations people overlook | Expectations can outpace what progressive loading can achieve | Some users overgeneralize “TB-500 fixes everything” narratives | Neither is a substitute for proper diagnosis and a loading plan |
My hands-on lesson: rehab logistics beat “which peptide is best”
In my own work with structured return-to-activity plans, the biggest difference-maker wasn’t whether the discussion centered on BPC-157 or TB-500. It was whether we could control the inputs: exact exercise selection, progression rate, and pain monitoring. I remember a case where two people were using different peptides, but the one who improved faster did so because:
- They reduced aggravating loading early
- They used progressive rehab and kept weekly measurable targets
- They didn’t restart high-intensity work the moment pain dipped
That experience shaped how I answer the question “is bpc 157 better than tb 500”: it depends on your injury pattern and your execution quality, not just the peptide name.
BPC-157: where it tends to fit best in real-world injury recovery
BPC-157 is commonly discussed as a recovery-support peptide, and many users approach it with the goal of helping tissues move through healing phases more effectively. In practice, it often comes up when someone has:
- Soft-tissue pain that feels persistent beyond the expected early recovery period
- Difficulty tolerating progressive loading without symptoms flaring
- A strong emphasis on “repair” and structured recovery scheduling
Why the “BPC-157 logic” appeals to rehab-focused people
What I see with people who choose BPC-157 is a tendency to treat it as part of a staged plan: symptom control first, then gradual stress exposure. That matters because connective tissues often need controlled mechanical stimulus during remodeling. If you choose BPC-157, your best chance at a meaningful signal is to pair it with:
- A staged strengthening plan (isometrics → assisted → progressive resistance)
- Pain-guided progression rules (e.g., don’t let symptoms climb week-over-week)
- Recovery support like sleep, hydration, and nutrition consistency
Limitations to acknowledge
Where I’ve seen people disappointed is when they treat BPC-157 like a “reset button.” If the underlying issue is biomechanics, inadequate tissue capacity, or incomplete rehab, symptom improvement can be partial or short-lived. In those cases, no peptide choice fully replaces the rehab problem.
TB-500: where it tends to fit best in real-world injury recovery
TB-500 is often discussed as another peptide option used for recovery and connective tissue support. In day-to-day conversations, TB-500 tends to be chosen by people who are looking for a connectivity/repair-oriented strategy and who believe it helps their recovery trajectory during training blocks.
Practical reasons users gravitate toward TB-500
From what I’ve observed in training and rehab logs, people choosing TB-500 often emphasize:
- Tissue resilience during return-to-exertion
- Managing persistent connective tissue discomfort
- A willingness to run a structured progression over time
Limitations to acknowledge
The common failure mode is overgeneralization: assuming TB-500 is automatically “better” for any injury type. If the problem is tendinopathy driven by load mismatch or technique, a peptide alone won’t fix training structure. The best results typically show up when TB-500 (or any peptide) is paired with load management and a long-enough rehab timeline to reach remodeling.
So… is BPC-157 better than TB-500?
The most accurate answer is: there isn’t a universal, one-size-fits-all winner. When someone asks “is bpc 157 better than tb 500,” the most useful way to think is in terms of:
- Injury type and tissue behavior: how your specific tissue responds to controlled loading
- Rehab stage: early irritation vs later remodeling and strengthening
- Execution quality: adherence to progressive programming and measurable milestones
- Trial clarity: whether you can track outcomes without changing multiple variables at once
A decision framework I’d actually use
- Diagnose the pattern: identify whether you’re dealing with a strain, tendinopathy, ligament irritation, or post-injury sensitivity.
- Pick one variable to learn from: if you’re trialing peptides, keep your rehab program consistent as much as possible.
- Choose measurable outcomes: range of motion, pain-free range, and the highest pain-limited load you can tolerate without flare-ups.
- Give the process time: avoid judging too early; connective tissue often requires weeks-to-months of progressive exposure.
Safety, sourcing, and “what I’ve learned about real-world implementation”
Before anyone runs a comparison in the real world, I recommend thinking about three practical realities:
- Quality control varies: peptide products from different suppliers can differ in formulation quality and consistency, which can muddy your results.
- Individual response varies: two people can run the same approach and experience different outcomes due to genetics, training load, and injury severity.
- Rehab determines the ceiling: if your program is flawed, your biological “support” won’t fully compensate.
I’m not going to pretend peptide selection alone guarantees a recovery outcome. In my hands-on experience, the best learning comes from tight tracking and disciplined rehab—not from choosing a winner based on forum threads.
FAQ
Is BPC-157 better than TB-500 for tendon recovery?
Not universally. In tendon problems, outcomes depend heavily on load management and a progressive tendon rehab program. If you’re trialing one, choose the one you can track alongside consistent rehab milestones, and avoid switching variables weekly.
How long should I wait before judging results from BPC-157 or TB-500?
For soft-tissue and tendon-related issues, it’s usually not a “days” decision. I’d base your judgment on a multi-week pattern of symptom response and your ability to progress loading without flare-ups, rather than a single early change.
Can I use both BPC-157 and TB-500 together to improve results?
Combining can make it harder to learn what’s working. If your goal is to answer “is bpc 157 better than tb 500” for your case, a cleaner approach is to keep your rehab consistent and run one variable at a time (when feasible) so your data isn’t confounded.
Conclusion: pick the right tool, then prove it with your rehab data
When people ask is bpc 157 better than tb 500, they’re really asking which approach fits their injury biology and their ability to execute rehab. In practice, BPC-157 and TB-500 are both discussed as recovery-support peptides, but the biggest drivers of outcomes are diagnosis accuracy, staged loading, measurable progression, and consistency.
Next step (actionable): Choose one peptide strategy (BPC-157 or TB-500), keep your rehab plan consistent for a defined period, and track 3 measurable milestones weekly—pain-free range, tolerated load, and functional return—so you can make a real decision based on your own response.
Discussion