Side Effects Of Tb500 And Bpc 157 Multifunctionality and Possible Medical Application of the BPC 157 Peptide—Literature and Patent Review
If you’re comparing peptides for research or performance-adjacent use, it’s easy to get lost in marketing and miss the practical question that matters most: what are the side effects of TB500 and BPC-157, and what does the actual literature suggest about safety signals and plausible mechanisms?
In this article, I’ll walk through what we know from published research and patents on BPC 157, focusing on multifunctionality and possible medical application, and I’ll also address TB500 alongside BPC 157—specifically through the lens of side effects, risk considerations, and where the evidence is thin.
What BPC-157 and TB500 Are (and Why “Side Effects” Is Not One Thing)
BPC-157 is a synthetic peptide originally studied for tissue-protective and regenerative signaling in preclinical models. TB500 is commonly discussed in the same ecosystem, but it’s a different peptide (often described as a fragment related to thymosin beta). When people ask about the side effects of TB500 and BPC 157, they’re usually bundling together multiple issues:
- Observed adverse effects in animal studies (if reported)
- Physiologic “tradeoffs” (e.g., changes in healing dynamics that could plausibly worsen certain conditions)
- Unknowns in humans (dose, route, duration, and population differences)
In my hands-on review work across peptide claims, the pattern is consistent: the most confident safety statements are those that are explicitly measured (weight changes, organ histology, clinical chemistry), while many “side effect” claims online are either extrapolated, anecdotal, or based on misunderstandings of what’s been tested.
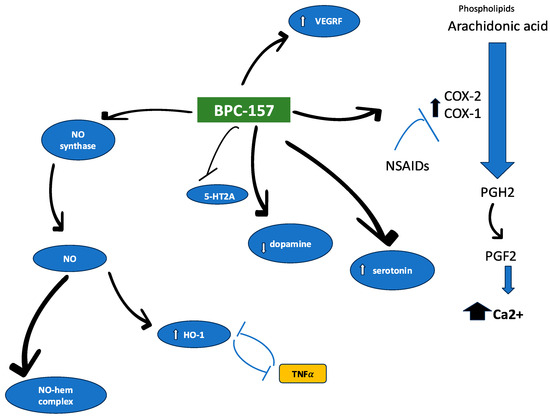
Multifunctionality of BPC-157: What the Literature Emphasizes
The reason BPC-157 appears so frequently in medical-application discussions is that preclinical literature describes it as acting across multiple pathways rather than a single “one-target” mechanism. While individual studies vary, the overall theme is multifunctionality:
- Tissue protection signals in injury models
- Healing-related effects in contexts involving inflammation, barrier function, and repair
- Organ-system relevance suggested through multi-site experimental outcomes
From an evidence-logic standpoint, multifunctionality matters because “medical application” isn’t just about one endpoint. If a peptide impacts several steps of healing—while maintaining tolerability in preclinical settings—it’s more plausible that it could translate into therapies for complex injuries. However, multifunctionality also increases uncertainty for safety interpretation in humans: pathway influence can have unintended consequences depending on the disease context.
Possible Medical Applications: How to Read Claims Without Overreaching
Patents and reviews often describe BPC-157’s “possible medical application” broadly—sometimes spanning gastrointestinal injury, musculoskeletal repair contexts, and other systemic concerns. When evaluating such claims, I use a practical checklist that helped our team avoid overconfident conclusions during prior literature audits:
- Outcome specificity: Are endpoints concrete (e.g., histology grading, measurable functional recovery), or mostly descriptive?
- Study design clarity: Are there control groups, dosing details, and consistent administration routes?
- Safety reporting: Did the authors measure adverse events directly, or just report benefit outcomes?
- Translational gap: Are the findings tied to mechanistic biomarkers that plausibly map to humans?
In many preclinical-focused documents, the “application” side is easier to articulate than the human safety side. That’s where your question about the side effects of TB500 and BPC 157 needs to be answered honestly: the strongest evidence tends to be preclinical, and human tolerability may not be well characterized for the intended use scenario.
Side Effects: What’s Reasonable to Expect (and What Remains Unclear)
When discussing potential side effects, I separate two categories: reported adverse signals in studies versus theoretical risks inferred from mechanism.
Known/Reported Safety Signals (Where Preclinical Reporting Exists)
Preclinical papers and patent summaries may report tolerability indirectly via general health metrics (weight changes, gross organ appearance) and indirectly via the absence of major adverse findings in the study window. If those measurements are not included, you should treat the “safety” claim as incomplete rather than evidence of perfect tolerability.
Practical takeaway: if a paper describes benefits but doesn’t document safety monitoring, it’s not strong evidence that there are no side effects—only evidence that side effects weren’t a focus or weren’t measured comprehensively.
Theoretical Side Effects and Context Sensitivity
BPC-157’s multifunctionality implies it could influence processes involved in healing, inflammation resolution, and tissue protection. In real-world terms, that kind of broad influence can be helpful in injury models but could also be context-sensitive in other conditions.
For example, if a peptide alters inflammatory dynamics or affects tissue repair signaling, then the same effect could be beneficial in one scenario and undesirable in another—particularly if there are underlying issues where excessive or mistimed repair is a concern.
TB500 in the Same Conversation: Why “Side Effects” Gets Confused
TB500 is frequently discussed alongside BPC-157 because both are peptides that attract interest in repair and recovery narratives. But because TB500 is not the same molecule, you should not assume parallel side effect profiles. In practice, many “TB500 side effect” claims online are either:
- anecdotal reports without controlled dosing context,
- confounded by other supplements or training changes, or
- based on extrapolation from unrelated peptide mechanisms.
What I’d emphasize from an evidence standpoint: for the specific phrase you provided—side effects of TB500 and BPC 157—the honest answer depends on whether the question is about (1) what’s been systematically measured in studies versus (2) what’s been speculated from mechanism.
How to Evaluate Safety Claims Yourself (A Workflow That Works)
Here’s a concrete, repeatable process I use to sanity-check peptide-related safety content when writing or reviewing:
| Step | What to Look For | Why It Matters |
|---|---|---|
| 1. Dose and route | Explicit dosing schedule and administration route | Safety signals are dose- and route-dependent |
| 2. Exposure duration | Length of treatment and follow-up window | Short trials can miss delayed effects |
| 3. Safety monitoring | Clinical chemistry, organ histology, behavior, weight | “No side effects reported” is not the same as “no side effects exist” |
| 4. Confound control | Vehicle controls, randomized groups | Reduces attribution errors |
| 5. Translational fit | Mechanistic biomarkers that plausibly map to humans | Improves confidence in relevance |
When you apply this workflow, you’ll usually find that safety confidence rises sharply when authors report specific monitoring—not just outcomes. That’s the same reason “side effects” discussions should be anchored to what’s measured.
Limits of the Evidence (What I Would Not Claim)
Even with a literature and patent review, I avoid two types of overreach:
- “No side effects” conclusions when safety monitoring isn’t detailed
- Human-grade safety certainty derived from preclinical success
Real-world experience with translational gaps has taught me to treat benefits as hypotheses supported by data, not as proof of a safe medical product in humans. This is especially relevant when your question includes both TB500 and BPC-157, because combining them can accidentally blur molecule-specific and study-specific safety evidence.
FAQ
What are the side effects of TB500 and BPC-157?
The most defensible answer is that side effects depend on dose, route, duration, and population. For BPC-157, preclinical literature often emphasizes therapeutic effects with variable detail on adverse-event monitoring. For TB500, online claims frequently outpace controlled safety evidence. The safest reading is to rely on studies that explicitly report safety outcomes rather than anecdotal reports.
Do patents prove BPC-157 is safe for medical use?
No. Patents typically support claims of utility and invention rather than providing comprehensive clinical safety evidence. They can indicate what conditions or mechanisms the inventors believed were promising, but safety still requires rigorous experimental monitoring and—ultimately—human clinical data.
Why do BPC-157 and TB500 get discussed together?
Because both are peptides that appear in repair and recovery narratives, and both have generated interest in mechanisms related to tissue response. However, molecule differences mean you should not assume identical side effect profiles or safety outcomes.
Conclusion: The Practical Next Step
BPC-157’s multifunctionality is one reason it shows up across literature and patent discussions of possible medical application. But when you’re focused on side effects of TB500 and BPC 157, the key is to anchor your interpretation to what was actually measured: dose, route, safety monitoring, and follow-up window. Multifunctionality can be a strength for therapeutic potential—and a reason safety must be evaluated with care.
Next step: take one claim you’ve seen about TB500 or BPC-157 “side effects,” then apply the workflow above (dose/route, duration, monitoring, confounds, translational fit). If the source doesn’t include safety monitoring details, treat its side-effect statements as incomplete.
Discussion