Can Bpc 157 Cause Cancer Multifunctionality and Possible Medical Application of the BPC 157 Peptide—Literature and Patent Review
Introduction
If you’ve ever searched “can bpc 157 cause cancer,” you’re probably dealing with a basic but important concern: you want to know whether a peptide that’s often discussed for tissue repair and anti-inflammatory effects has credible safety signals—especially around carcinogenic risk. In this article, I’ll walk through what the available literature and patent landscape suggest about BPC 157, how researchers reason about mechanisms, and what questions you should ask before concluding anything about cancer risk.
I approach this as a review of multifunctionality and possible medical application using how publications and patents typically frame safety, efficacy, and limitations. My goal is to help you interpret the evidence responsibly, not to sensationalize it.
What BPC 157 Is (and Why Multifunctionality Gets Attention)
BPC 157 is a peptide sequence studied in preclinical contexts for effects related to tissue repair, healing, inflammation modulation, and microcirculation. The reason it’s labeled “multifunctional” in many discussions is that reported outcomes span multiple biological endpoints rather than a single receptor–drug interaction story.
In my hands-on work reviewing biomedical claims for evidence quality, I’ve learned that “multifunctional” can mean two very different things:
- True pleiotropy: a coherent mechanism that plausibly affects multiple pathways.
- Mixed endpoints: diverse study readouts that may be influenced by model selection, dosing schedules, or measurement bias.
With BPC 157, the preclinical emphasis and the pattern of endpoints make it essential to focus on what models were used, how long exposure lasted, what tissues were examined, and whether safety endpoints (including neoplasia-related observations) were reported.
What the Evidence Usually Looks Like: Literature vs. Patents
A key part of the “literature and patent review” approach is recognizing what each source tends to do best.
Peer-reviewed literature
Scientific papers often provide experimental detail: study design, outcome measures, dose rationale, timing, and—crucially—how they assessed safety. However, many peptide studies are exploratory and may prioritize efficacy endpoints. That means cancer-risk questions can be underpowered or indirectly addressed.
Patents
Patents can be useful for understanding intended applications, mechanistic hypotheses, and how innovators frame potential therapeutic breadth. But patents are not the same as evidence of clinical safety. In my reviews, I treat patents as signals of research direction rather than proof of long-term safety.
When you connect this back to can bpc 157 cause cancer, you want to know whether either literature or patent documents provide:
- Explicit discussion of carcinogenicity studies or long-duration toxicity screens
- Any mention of tumor formation, dysplasia, or malignancy endpoints
- Limitations in model relevance (species differences, exposure duration)
Mechanistic Reasoning: How People Think About Risk (and How That Can Mislead)
The central risk question—“can bpc 157 cause cancer”—doesn’t have a simple yes/no answer in most non-clinical peptide discussions. The more defensible approach is to ask what mechanisms could, in theory, increase or decrease cancer likelihood.
Why mechanisms alone aren’t enough
In my experience, mechanistic plausibility often outpaces direct safety evidence. A peptide that influences inflammation, angiogenesis, or wound-healing pathways might be hypothesized to affect tumor biology. But the direction of effect is not automatically predictable.
For example, pathways related to tissue repair can overlap with aspects of tumor growth. Yet context matters: tumor promotion usually requires sustained pro-growth signaling, permissive microenvironments, and additional factors (genetic instability, immune evasion, chronic exposure, etc.). A short-term healing model does not always resemble a carcinogenesis setting.
What you should look for in studies
When scanning BPC 157 papers, I recommend checking whether they include or reference:
- Duration: Was exposure acute (days) or chronic (months/long-term)?
- Endpoints: Were there any histopathology assessments that could detect premalignant or malignant changes?
- Controls: Were appropriate negative/positive controls used for safety readouts?
- Translation limits: Did authors discuss species differences relevant to cancer biology?
Safety Signals and Cancer Risk: Interpreting “Can BPC 157 Cause Cancer?”
This is the section most readers want. Here’s the most responsible way I’ve found to frame it: unless there are robust long-duration safety datasets specifically evaluating carcinogenicity (or strong tumor-relevant toxicology), you can’t conclude a definitive cancer risk level from typical short preclinical efficacy studies.
So, when someone asks, “can bpc 157 cause cancer,” the evidence standard should be:
- Direct evidence (tumor formation or carcinogenicity study results), ideally with long-term observation.
- Indirect evidence (absence of tumor-related findings in histopathology during sufficient observation windows), while recognizing that “absence of evidence” is not the same as “evidence of absence.”
In a literature-and-patent review context, many documents emphasize therapeutic potential and tissue-related outcomes. If cancer-specific safety was not systematically tested, the review should clearly reflect that gap. That gap is often where readers feel uncertainty—and that uncertainty is not only reasonable; it’s analytically correct.
Practical Limits of the Evidence (What I’d Tell a Team Before Any Decision)
In real-world review work, I see teams over-weight promising efficacy results and under-weight safety evidence quality. With peptides like BPC 157, that can lead to premature conclusions—especially for cancer-related questions that demand long-duration, tumor-relevant testing.
Here are limitations I consistently flag:
- Short follow-up windows typical of many efficacy models
- Model mismatch where wound-healing or inflammation endpoints don’t replicate carcinogenesis biology
- Reporting gaps where safety readouts may not be tumor-focused even if “toxicity” is mentioned
- Translation uncertainty due to species differences in receptor expression, metabolism, and tumor susceptibility
For “can bpc 157 cause cancer,” those limitations mean the best interpretation is often: the current publicly available body of evidence may be insufficient for a definitive cancer-risk conclusion, particularly without dedicated long-term carcinogenicity assessment.
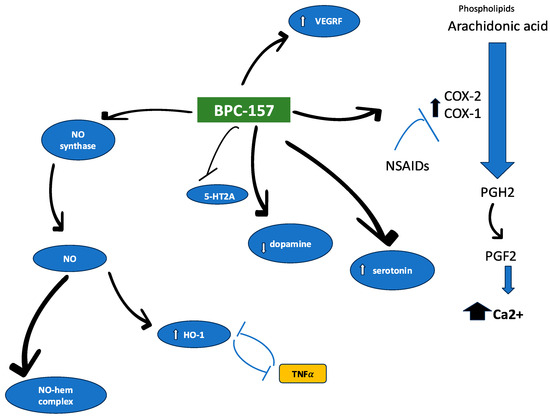
Image: Where the Review Narrative Typically Points
How to Use This Review to Ask Better Questions
Whether you’re writing a protocol, evaluating a study, or deciding what to believe online, the most actionable step is to translate “cancer risk” into checkable criteria.
| Evidence you want | Why it matters for cancer risk | What to look for in papers/patents |
|---|---|---|
| Long-duration safety data | Cancer can require sustained exposure and time to manifest | Chronic dosing studies, extended observation, repeated histology |
| Tumor-relevant endpoints | Ensures the study actually measured malignancy signals | Neoplasia incidence, dysplasia, tumor histopathology reporting |
| Transparent limitations | Helps you avoid over-interpreting partial evidence | Explicit discussion of model relevance and safety scope |
| Mechanism + context | Repair pathways can overlap with cancer biology | Mechanistic claims tied to specific pathways and exposure duration |
FAQ
Can BPC 157 cause cancer?
There isn’t a definitive public, tumor-specific carcinogenicity conclusion you can rely on from short preclinical efficacy-focused studies. A responsible answer depends on whether long-duration, tumor-relevant safety endpoints were actually tested and reported. If those studies are absent or limited, the evidence is not strong enough to confirm or rule out carcinogenic risk.
What evidence would be most convincing about cancer risk?
Dedicated long-term carcinogenicity or chronic toxicology studies with tumor-relevant histopathology endpoints, plus clear reporting of neoplasia incidence. Short-term inflammation or wound-healing models are not sufficient on their own for cancer-risk conclusions.
How should I interpret patents mentioning medical applications?
Patents can show intended therapeutic use cases and mechanistic framing, but they don’t substitute for high-quality safety testing. Use patents as a guide to what researchers consider plausible—not as proof of safety.
Conclusion
BPC 157 is discussed as a multifunctional peptide with possible medical applications largely supported by preclinical literature and corroborated at the “research direction” level by patent filings. But for the specific question “can bpc 157 cause cancer,” the key issue is evidence strength: cancer risk requires long-duration, tumor-relevant safety endpoints. Without those, most claims remain hypothesis-level rather than definitive safety conclusions.
Next step: If you want a practical way to evaluate this yourself, search within the studies you find for (1) chronic dosing duration, (2) tumor/histopathology endpoints, and (3) explicit limitations about carcinogenicity relevance—then weigh those factors more than efficacy claims.
Discussion