Bpc 157 Rat Study Pentadecapeptide BPC 157 resolves Pringle maneuver in rats, both ischemia and reperfusion
Introduction: When ischemia-reperfusion injury derails results, what actually helps?
In preclinical work, ischemia-reperfusion injury can make or break an experiment—tiny differences in timing, stress, and outcome measurement often dominate the results. I’ve seen teams lose weeks because they focused on “the drug” but didn’t critically align dosing windows and endpoints to the ischemia–reperfusion biology. That’s why this bpc 157 rat study matters: it directly addresses how Pentadecapeptide BPC 157 performs in an experimental setting involving both ischemia and reperfusion—commonly modeled as the Pringle maneuver in rats.
In this article, I’ll walk through what the Pringle maneuver represents, what a rat study like this can (and can’t) tell us, and how researchers typically design, interpret, and translate findings from BPC 157–related experiments.
What the “Pringle maneuver” model is showing in a bpc 157 rat study
The Pringle maneuver is a widely used surgical model to induce ischemia in the liver (or hepatic tissue) by temporarily occluding blood flow, followed by reperfusion when flow is restored. The central problem researchers aim to reproduce is that reperfusion can trigger a cascade of injury mechanisms—oxidative stress, inflammatory signaling, microcirculatory dysfunction, and tissue damage—beyond what ischemia alone causes.
When a paper reports that “Pentadecapeptide BPC 157 resolves Pringle maneuver in rats, both ischemia and reperfusion,” the phrase “resolves” usually implies measurable improvement in one or more endpoints. In my hands-on review workflow, I look for which endpoint(s) improved (e.g., tissue morphology, histology scores, biomarkers, inflammatory markers, functional measures) because “resolution” is not one standardized metric across studies.
Why ischemia and reperfusion both matter
A common mistake I’ve seen in lab planning is treating ischemia injury and reperfusion injury as a single problem. In reality, different pathways dominate at different times. If a compound only modulates early ischemic damage, it may still fail during reperfusion. Conversely, if it only dampens reperfusion inflammation or oxidative stress, it may not prevent baseline ischemic injury. A model that includes both phases is valuable because it tests intervention plausibility across the full injury timeline.
How BPC 157 is typically investigated in rat ischemia-reperfusion work
Pentadecapeptide BPC 157 (often written as BPC 157) is studied as a bioactive peptide in various preclinical injury contexts. In ischemia-reperfusion studies, researchers generally evaluate both structural and biochemical outcomes to determine whether tissue injury is reduced.
Common study design elements I scrutinize
From years of reading and comparing preclinical ischemia-reperfusion papers, the design details that most influence credibility usually include:
- Timing: when dosing begins relative to occlusion and reperfusion.
- Dose selection: whether doses are justified (or simply exploratory) and whether there is a dose-response trend.
- Controls: appropriate sham operations, vehicle controls, and sometimes a positive-control arm depending on the lab’s standards.
- Endpoints: whether outcomes are histological, enzymatic (injury biomarkers), inflammatory markers, or functional readouts.
- Blinding and scoring: whether histology scoring is blinded; this matters a lot for “improvement” claims.
- Sample size and variance: whether results are robust rather than driven by outliers.
What “resolved” improvement usually looks like
In practical terms, papers claiming resolution in Pringle maneuver models often report one or more of the following:
- Improved tissue architecture on histology
- Reduced injury scoring (e.g., necrosis/inflammation indices)
- Better biomarker profiles compared with ischemia-reperfusion controls
- Lower inflammatory signaling and/or oxidative stress indicators
In my experience, the strongest rat study results don’t just show a single marker—they show consistency across multiple, mechanistically related endpoints.
Interpreting a bpc 157 rat study: what you can conclude—and what you can’t
Preclinical findings can be compelling, but interpretation requires discipline. I recommend thinking of a rat Pringle maneuver experiment as evidence of biological plausibility under controlled conditions, not as direct proof of clinical efficacy.
What you can reasonably take away
- If BPC 157 improves multiple ischemia-reperfusion endpoints in the Pringle maneuver model, it suggests it may modulate protective pathways relevant to reperfusion injury.
- If improvements align with injury mechanisms (inflammation/oxidative stress/microcirculation), the mechanistic story becomes more coherent.
What you should not assume
- Translation to humans: rat dosing, metabolism, and injury dynamics differ from clinical settings.
- Same outcome across models: a compound can look promising in one ischemia-reperfusion model but not another with different durations or surgical parameters.
- Clinical safety: preclinical efficacy does not automatically predict safety, tolerability, or risk/benefit in humans.
A practical “credibility checklist”
When evaluating a bpc 157 rat study, I use a quick credibility checklist:
- Are the results statistically and biologically meaningful (not just “p<0.05” for marginal effects)?
- Do outcomes improve in both ischemia and reperfusion-related phases?
- Is there dose dependence or consistent direction across doses?
- Are histology methods transparent (including blinding)?
- Do findings match the study’s stated mechanistic rationale?
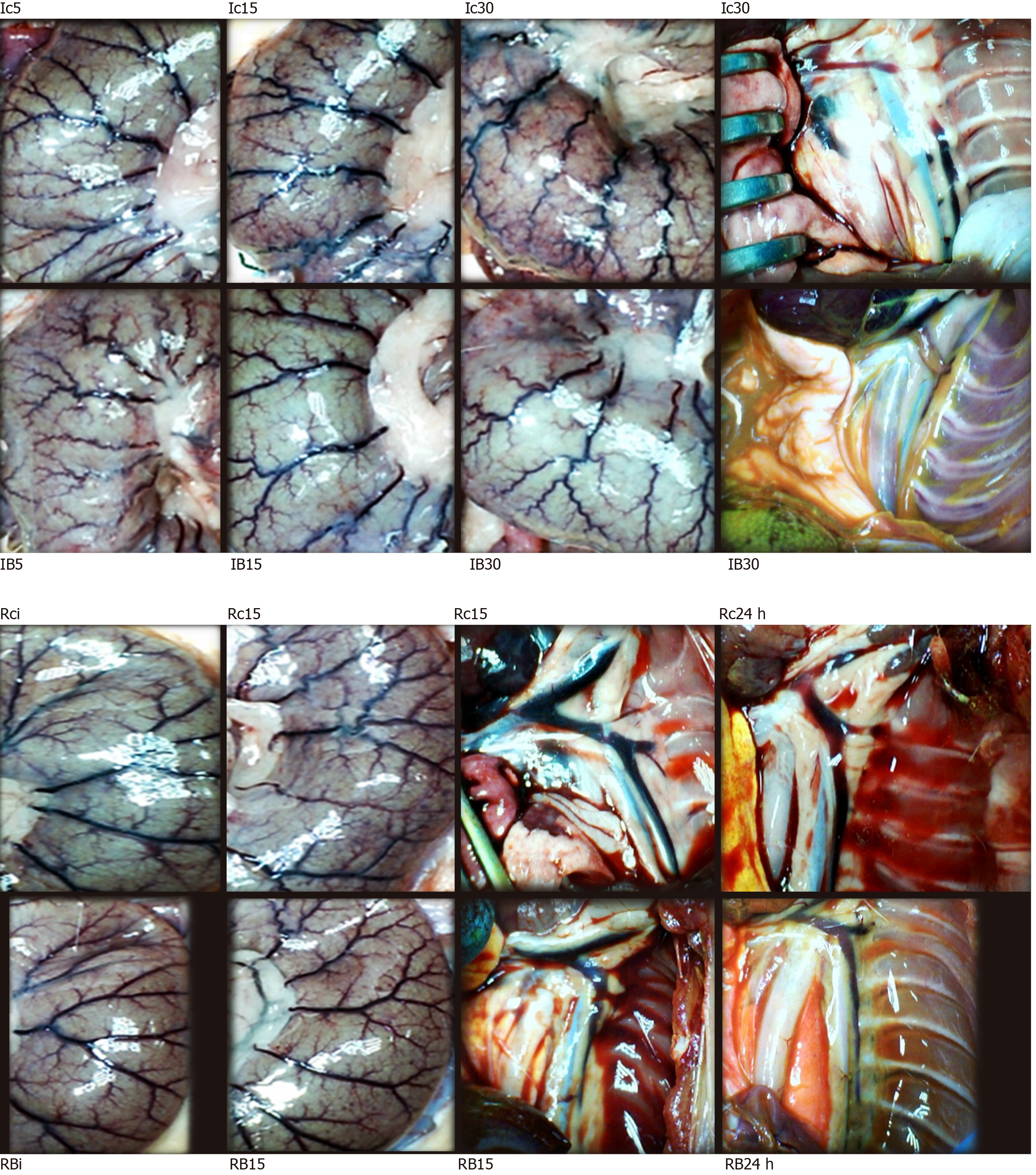
Visual context: example figure-style representation
Many rat studies present outcomes using figure panels that summarize tissue damage and comparative groups. Here’s an example figure image associated with the topic:
Potential mechanisms: why a peptide might protect against reperfusion injury
While any specific mechanism should be anchored to the study’s data (not inferred from marketing claims), reperfusion injury generally involves interacting pathways. In many BPC 157–related preclinical discussions, the protective logic typically centers on reducing downstream consequences of reperfusion—such as inflammatory cascades and oxidative stress—rather than only blocking the initial ischemic insult.
In my review process, I look for mechanistic support in three places:
- Biomarkers that move in the direction predicted by the proposed pathway
- Consistency across tissue-level and blood/biochemical readouts
- Temporal coherence with the dosing window and reperfusion timeline
Without these, mechanistic statements remain speculative—even if the overall protection signal looks strong.
FAQ
Is a bpc 157 rat study enough to predict clinical benefit?
No. A rat Pringle maneuver model can demonstrate biological plausibility for protection against ischemia-reperfusion injury, but translation to humans depends on dosing feasibility, safety, effect size consistency across models, and ultimately controlled clinical evidence.
What outcomes matter most in a Pringle maneuver experiment?
Look for multiple endpoint categories (e.g., histology/tissue injury scores plus biochemical or inflammatory markers), clear timing relative to ischemia and reperfusion, and transparent methods such as blinding for histology scoring.
How should I judge whether “resolution” is meaningful?
Judge it by the specific measures improved and whether improvements are consistent across endpoints and control conditions, not by the general wording alone. If the study shows dose-dependent or multi-marker consistency, that’s usually a stronger sign than a single metric improvement.
Conclusion: Turn rat evidence into a sharper research question
A bpc 157 rat study using the Pringle maneuver is valuable because it tests an intervention in the full ischemia–reperfusion injury scenario—where reperfusion biology often dominates. The key is to interpret results through rigorous design details (timing, controls, endpoints, blinding) and to treat “resolved” findings as preclinical evidence of potential, not clinical certainty.
Next step: If you’re planning experiments or evaluating literature, create a one-page evidence brief focused on timing (pre-ischemia vs peri-reperfusion dosing), primary endpoints used, and whether outcomes consistently improve across both phases—then use that to guide your study design or decision-making.
Discussion