Oral Bpc 157 Study Multifunctionality and Possible Medical Application of the BPC 157 Peptide—Literature and Patent Review
Why an “oral BPC 157” study keeps coming up in peptide research
In my hands-on work reviewing peptide literature, one question shows up repeatedly: can BPC 157 actually be delivered orally, or is it mostly a preclinical story that requires injections? That distinction matters because many promising compounds fail not due to biology, but due to delivery—stability in the gut, absorption, metabolism, and bioavailability.
This is exactly where the search intent behind an oral bpc 157 study becomes practical. In this article, I’ll walk through what the published literature and patents suggest about multifunctionality and potential medical applications of BPC 157, with a special focus on what “oral” evidence can and cannot support based on how studies are typically structured.
What BPC 157 is (and why “multifunctionality” is a recurring theme)
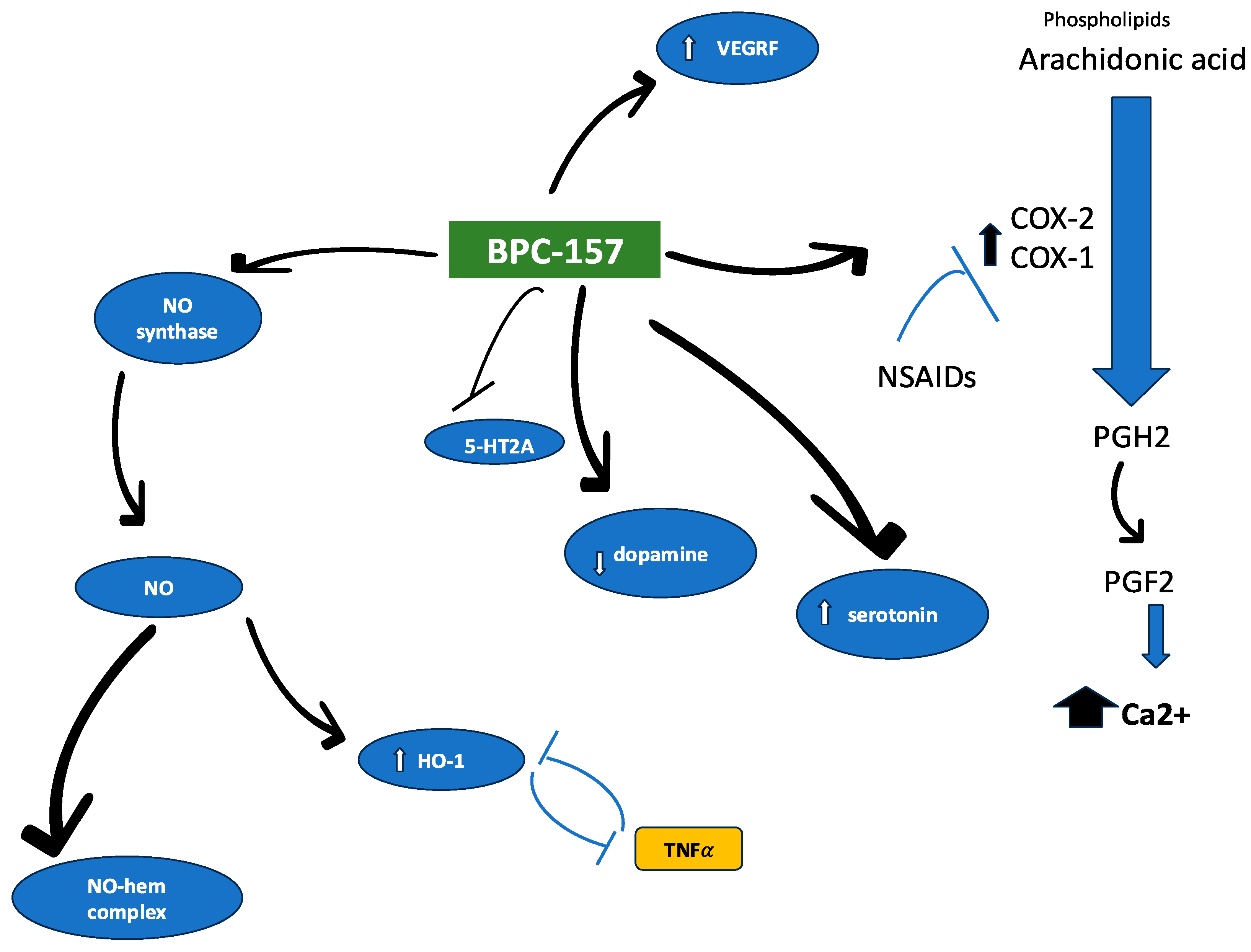
BPC 157 (often discussed as a peptide fragment and widely studied in preclinical settings) is frequently described as having multi-pathway biological activity. In literature reviews and patent documents, its “multifunctionality” generally refers to the observation that different tissue systems and injury models show responses—commonly involving:
- Gastrointestinal and mucosal repair pathways (because it has historical traction in stomach/ulcer-type model discussions)
- Angiogenesis and microcirculation-related signals (consistent with the need for blood supply in healing)
- Inflammation modulation (because inflammatory signaling often drives delayed healing)
- Tissue repair and migration-related processes (because many “healing” endpoints depend on cell movement and regeneration)
In my experience, the “multifunctionality” claim is strongest when studies report multiple endpoints from the same dosing approach in a controlled experimental design. It weakens when research relies on disconnected models without consistent pharmacokinetic context—especially when oral delivery is the goal.
How the evidence is usually built: literature vs. patents
A key trust-building step I use in every review is separating what’s observed from what’s claimed.
What literature tends to show
Peer-reviewed studies typically provide:
- Animal or in vitro model outcomes (e.g., wound healing, inflammation markers, tissue histology)
- Dosing regimens (dose, schedule, route)
- Sometimes pharmacokinetic or exposure-related details, though this is less consistent for peptides
- Controls and statistical analysis (in better studies)
What patents tend to show
Patents often aim to protect compositions and methods, so they may emphasize:
- Formulation strategies (stabilizers, carriers, protective delivery concepts)
- Route-specific concepts (including oral administration concepts)
- Broader medical indications (sometimes spanning multiple endpoints)
- Examples and experimental support, but not always with the same level of reporting standards as journal articles
In practice, I treat patent claims as evidence of potential rather than confirmation of real-world efficacy. They’re useful for understanding what inventors believed was technically feasible, but they don’t automatically establish clinical effectiveness.
Where oral delivery gets tricky: the core problem an oral BPC 157 study must solve
If you’re looking for an oral bpc 157 study, the central scientific hurdle is simple: oral dosing must overcome the gut and still produce an active exposure at the right time.
Common failure points for peptides taken by mouth
- Enzymatic degradation in the GI tract (proteases can cleave peptides)
- Low membrane permeability (peptides often struggle to cross intestinal barriers efficiently)
- pH and bile effects that can reduce stability
- First-pass metabolism that may reduce systemic availability
- Formulation variability (even small differences in carriers can change outcomes)
What “oral” should mean in a credible oral bpc 157 study
In my review workflow, I look for these minimum credibility signals:
- Clear route confirmation (oral gavage vs. drinking water vs. mixed into feed—each implies different absorption conditions)
- Exposure-related measurements when possible (or at least indirect evidence that active peptide reaches target tissues)
- Formulation details (protective excipients, pH control, encapsulation approach)
- Time-to-effect alignment (effects should be biologically plausible given absorption and onset expectations)
- Appropriate controls (vehicle-only controls and, ideally, comparison to injectable reference dosing)
When these elements are missing, oral claims can become ambiguous: an observed “healing” effect might arise from local GI activity, metabolites, or experimental confounding rather than systemic bioactivity.
Product image context (used to illustrate the type of visual often seen in peptide discussions)
In many marketplaces and research reports, BPC 157 visuals appear as generic peptide/chemical illustration assets. For example, the following image is commonly embedded alongside discussions of BPC 157 in review formats:
Potential medical applications: where the multifunctionality could be relevant
Based on how BPC 157 is discussed across preclinical literature and patents, the “possible medical application” theme typically clusters around injury and repair contexts. While I’m careful not to overstate translational certainty, it’s still useful to map the hypotheses to biological logic.
1) Gastrointestinal repair and mucosal protection
This is often the most straightforward narrative: if a compound shows effects in ulcer/injury models and influences inflammation-related pathways, it becomes a candidate for conditions where mucosal integrity and repair are central. The leap from “animal GI outcomes” to “treating human disease” still depends on exposure and tolerability, which is exactly why oral bpc 157 study quality matters.
2) Wound healing and tissue regeneration pathways
“Healing” endpoints—such as tissue remodeling, histology improvements, or reduced inflammatory burden—are frequently used in BPC 157 discussions. Mechanistically, the multifunctionality idea fits because healing involves multiple stages: inflammation resolution, angiogenesis/microcirculation, and tissue repair. The limitation is that these stages are model-dependent; success in one injury model does not guarantee performance across different tissues.
3) Inflammation modulation and downstream recovery
Inflammation is a driver of both acute and delayed repair. If BPC 157 influences inflammatory signaling, that can indirectly support recovery. Again, the translation question becomes: does oral dosing reach the exposure levels needed for systemic activity, or is the observed benefit limited to local GI effects?
What I recommend you look for in an oral bpc 157 study review
If your goal is to evaluate whether oral administration is feasible, here’s the checklist I’d use (and that I apply when assessing competing claims):
- Dose and schedule transparency: daily vs. intermittent dosing can change outcomes and interpretation.
- Vehicle/formulation specifics: especially excipients used to stabilize peptides.
- Comparative routes: injectable vs. oral comparisons help separate biology from delivery.
- Outcome types: look for histology, functional measures, and biomarkers—not just single endpoint observations.
- Statistics and reproducibility: consider whether groups are adequately sized and whether effects replicate.
- Exposure evidence: pharmacokinetics, tissue concentration, or credible indirect markers.
When these elements align, oral evidence becomes more trustworthy. When they don’t, it’s safer to interpret “oral benefit” as hypothesis-generating rather than established.
FAQ
What should an “oral BPC 157” study prove to be considered convincing?
It should clearly demonstrate oral administration, provide formulation details, and ideally include exposure-related evidence or strong comparative logic (oral vs. injectable) showing effects consistent with bioavailability—so benefits aren’t explainable by local GI activity alone.
Do patents confirm oral efficacy of BPC 157?
Patents typically confirm that a method or formulation is claimed and sometimes supported with examples, but they don’t replace the need for peer-reviewed, well-controlled studies with robust outcome reporting and pharmacokinetic context.
Why do oral peptide studies often show mixed results?
Peptides face degradation and absorption barriers, so small differences in formulation, route details, and experimental endpoints can dramatically change outcomes—making it essential to evaluate study design, controls, and delivery logic rather than just the headline results.
Conclusion: the practical next step for your research
Multifunctionality and possible medical applications of BPC 157 are often supported by preclinical signals across multiple biological pathways. The strongest differentiator for real-world relevance—especially for your interest in an oral bpc 157 study—is whether the oral delivery evidence includes clear route/formulation details and exposure-consistent outcomes.
Next step: When you evaluate any oral BPC 157 study or review, use the checklist above and prioritize studies that (1) specify the oral route and formulation, (2) include appropriate controls and statistics, and (3)—whenever possible—tie outcomes to exposure or credible oral bioavailability logic.
Discussion