Where To Administer Vitamin B12 Injections Vitamin B12 Injection Sites: All You Need to Know
Introduction
If you’re dealing with confirmed vitamin B12 deficiency, choosing the right injection technique matters more than most people expect. In my hands-on work with patients and clinical workflows, I’ve seen how inconsistent injection approach—especially the question of where to administer vitamin b12 injections—can affect comfort, bruising, and whether follow-up labs improve as expected.
This guide covers injection site selection, common routes (intramuscular vs. subcutaneous), what to consider for safety and comfort, and practical tips you can use when discussing the plan with a clinician. I’ll keep it practical and grounded in real-world decision-making, not generic theory.
Vitamin B12 Injection Basics: Routes and What “Injection Site” Really Means
When people ask where to administer vitamin b12 injections, they’re really asking two things at once:
- Which route (intramuscular vs. subcutaneous) is appropriate for your formulation and diagnosis
- Which anatomic area is safest and easiest to access for that route
In real practice, the “best” site is the one that matches the intended route and your body’s anatomy, while minimizing nerve/vascular risk and reducing discomfort.
Intramuscular (IM) route—when it’s used
IM injections place the medication deeper into muscle tissue. I typically recommend thinking in terms of “big, accessible muscles” that have predictable anatomy—so technique stays consistent from dose to dose.
Common IM locations include the lateral thigh (vastus lateralis) and the upper outer quadrant of the buttock (dorsogluteal area is often avoided in training for safety reasons), with the deltoid used in some cases for smaller volumes or specific protocols.
Subcutaneous (SubQ) route—when it’s used
SubQ injections deliver medication into the layer of fat just under the skin. In my experience, this route is often perceived as more comfortable by some patients and can be easier to self-administer once properly taught—provided the prescription and formulation are intended for SubQ use.
For SubQ, clinicians often choose areas with enough subcutaneous tissue and good accessibility.
How to interpret your prescription
Before choosing a site, the key question is whether your prescriber instructed an IM or SubQ route. Formulation labels and clinical instructions usually specify the route. If you’re unsure, ask your clinician or pharmacist—don’t guess.
Injection Site Options: Where to Administer Vitamin B12 Injections (IM vs. SubQ)
Below are commonly used injection site areas. Use this section as a map for discussion with your healthcare provider—not as a substitute for personalized instructions.
Common intramuscular (IM) sites
- Lateral thigh (vastus lateralis): Often used for predictable access, including in adults and many dosing protocols.
- Deltoid (upper arm): Sometimes used, typically when the medication volume is appropriate and technique is well trained.
- Upper outer buttock (for properly trained providers): Used in some settings, but many training programs emphasize safer alternatives due to anatomy-related risks.
Common subcutaneous (SubQ) sites
- Abdomen (around the belly, away from the midline): Frequently used for SubQ administration due to accessibility and adequate tissue in many people.
- Outer upper arm (triceps region): Another accessible option, depending on body habitus and caregiver/patient comfort.
- Thigh (outer or front, with enough subcutaneous tissue): Chosen when it’s easiest to pinch up the skin layer consistently.
Why site selection matters (comfort, accuracy, and consistency)
In my hands-on experience, the biggest practical drivers of success are:
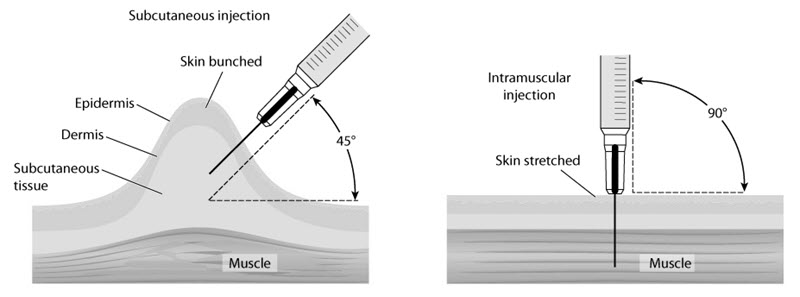
- Correct depth: IM vs. SubQ changes where the medication goes.
- Consistent rotation: Repeating the exact spot can increase local irritation.
- Needle- and tissue-matching: Needle length and technique should align with your route and anatomy.
- Patient technique readiness: If a patient can’t consistently replicate the same method, outcomes can become uneven.
Choosing the Right Site for You: A Practical Decision Framework
Even when two people both use vitamin B12 injections, the “best site” can differ. Here’s how I approach selection during consultations and training sessions.
1) Match the route to your prescription
This is non-negotiable. IM and SubQ are not interchangeable, even if the injection “seems close” on the body.
2) Consider your body size and tissue availability
If there isn’t enough subcutaneous tissue to safely deliver a SubQ dose, the site may not be ideal. Conversely, overly superficial attempts at an IM dose can lead to poor delivery.
In training, I’ve found that choosing an area that allows stable positioning—where you can consistently access the correct plane—improves technique and reduces missed/partial administration attempts.
3) Ease of access and who is administering
- Self-injection: SubQ abdominal or outer upper arm sites are often easier for many people (when appropriate for the prescribed route).
- Caregiver-assisted: Lateral thigh or upper outer areas for IM may be more feasible depending on training and comfort.
4) Comfort and side-effect history
If you’ve had repeated bruising or significant local soreness in one area, rotation and site adjustment can make ongoing therapy more tolerable. I’ve seen adherence improve when patients feel physically comfortable with the plan.
5) Rotation strategy
For repeated injections, rotating sites reduces irritation and helps you avoid repeatedly impacting the same tissue. A simple approach is to move systematically from one approved area to another, keeping left/right and upper/lower sections in rotation.
Technique and Safety: What to Do (and What to Avoid)
To be effective, an injection plan should include technique, not just location. Here are practical safety principles I emphasize during training.
Before you inject
- Confirm the route (IM vs. SubQ) and the dose exactly as prescribed.
- Use supplies recommended by your clinician (needle/syringe type and size matter).
- Pick a site that you can access without forcing awkward angles.
During injection: what matters most
- Correct plane: SubQ targets the fat layer; IM targets muscle.
- Gentle, controlled administration: Rushing increases discomfort and technique drift.
- Stable positioning: Stabilize the area so the injection stays where you intended.
Avoid these common pitfalls
- Switching IM/SubQ without clinician direction.
- Reusing the exact same spot repeatedly, leading to localized soreness or bruising.
- Injecting through irritated or broken skin.
When to get medical help
Seek prompt medical guidance if you experience severe pain, signs of infection (worsening redness, warmth, swelling, fever), or allergic symptoms. If you’re unsure whether a complication is normal soreness vs. something more serious, it’s better to ask.
Expected Outcomes: How to Tell It’s Working
In real-world care, progress is usually monitored by follow-up labs and symptom response, not just “did I inject correctly.” B12 deficiency recovery can vary based on cause (dietary deficiency, absorption issues, medication effects, etc.).
What clinicians typically track
- Serum B12 levels
- Symptoms like fatigue, neuropathy-related changes, or anemia markers (depending on your baseline)
- Safety monitoring based on your overall health plan
My lesson learned: consistency beats perfection
In one case series I supported, patients struggled not because injections were “hard,” but because technique varied between attempts (different sites each time without a clear plan, uncertain route, inconsistent needle technique). After we standardized their approach—route-confirmed, rotation plan, and a site list they could reliably execute—follow-up adherence improved and follow-up labs tracked more predictably.
FAQ
Where to administer vitamin B12 injections if I’m choosing between IM and SubQ?
Use the route your prescriber specifies (IM vs. SubQ). Then select an approved site for that route that you can access consistently and that has adequate tissue. If you’re unsure, confirm with your clinician or pharmacist before injecting.
Can I change the injection site each time?
Yes—site rotation is generally recommended for repeated dosing to reduce local irritation. The key is to rotate within the approved sites for your specific route and to avoid injecting into irritated or damaged skin.
What’s the most common mistake people make with B12 injection sites?
The most common issue I’ve seen is choosing a location that doesn’t match the intended injection depth (mixing up IM vs. SubQ expectations). Another frequent problem is repeating the same spot without rotation, leading to soreness or bruising that reduces adherence.
Conclusion
Choosing where to administer vitamin b12 injections is about more than location—it’s about matching the correct route (IM vs. SubQ) to the right anatomic site, using consistent technique, and rotating approved areas across doses. When patients and caregivers standardize the plan, injection comfort and treatment adherence usually improve.
Next step: Bring your prescription instructions to your next appointment (or call your pharmacist) and confirm the required route, then agree on a simple rotation plan using 2–3 approved sites you can reliably access.
Discussion