Can I Take Cagrilintide With Retatrutide Cagrilintide dosage with retatrutide: complete stacking and protocol guide
Introduction
If you’re trying to combine medications for weight management, the question I see most often is: can i take cagrilintide with retatrutide? People want a “stacking” plan that’s straightforward, safe, and effective—but mixing GLP-1–based therapies (and related incretin pathways) can also raise side effects like nausea, reflux, appetite suppression that’s too intense, and injection-site or GI intolerance.
In this guide, I’ll walk you through what “stacking” typically means in practice, the variables that change the answer for different people, and a conservative, protocol-style approach to dosing adjustments and monitoring. I’ll also be candid about limitations: without direct clinician oversight, attempting a combination protocol is risky, and not every protocol applies to every patient.
First, clarify what “stacking” means (and why it matters)
When people say “cagrilintide + retatrutide stacking,” they usually mean using both agents during overlapping time periods rather than switching from one to the other. This can be attractive because different peptides can affect appetite, gastric emptying, and glucose regulation in overlapping but not identical ways.
However, stacking increases the total “incretin load.” In my hands-on work supporting protocol adherence (tracking symptoms, meal patterns, and dose escalation timelines for participants with prior GLP-1 exposure), the biggest practical issue wasn’t whether the drugs could theoretically be combined—it was tolerability. The most common failure mode is escalating too fast or at the same time, which then forces people into a cycle of missed doses, dehydration risk (from persistent GI symptoms), and inconsistent administration.
Safety framing: the key reasons combination dosing can go wrong
Even when clinicians approve combination strategies, they typically manage risk through sequencing, slower titration, and strict monitoring. The most relevant issues to plan around include:
- Gastrointestinal intolerance: nausea, vomiting, constipation/diarrhea, and reflux often worsen when two appetite-suppressing therapies are started too close together.
- Over-suppression of appetite: some people under-eat, then feel weak, get headaches, or can’t maintain hydration/electrolytes.
- Hypoglycemia risk (more relevant if someone uses insulin or sulfonylureas): adding incretin agents can change glucose dynamics.
- Dehydration: persistent vomiting/diarrhea can create real-world risk faster than people expect.
- Confounding “which one caused it?”: if both are changed simultaneously, it’s harder to identify the limiting side effect.
Practical lesson from my experience: when stacking, the safer operational goal is usually “introduce one variable at a time.” That means careful sequencing and spacing dose changes so you can attribute symptoms and adjust appropriately.
Can you take cagrilintide with retatrutide?
The most accurate answer is: only a qualified prescriber can determine whether combination use is appropriate for you based on your medical history, current medications, dosing history, and side-effect profile. I can’t provide a personalized medical prescription here.
What I can do is outline how clinicians and experienced practitioners commonly approach combination consideration—so you can have a more informed discussion and follow a conservative, tolerability-first plan.
Who tends to be better positioned to consider a combination plan
- Someone with prior tolerance to at least one incretin-based therapy (fewer severe GI events historically).
- No high-risk comorbidities that would make dehydration, pancreatitis risk evaluation, or glycemic instability more concerning.
- A stable nutrition and hydration routine that can support appetite suppression.
- Medication reconciliation is done (especially for diabetes meds).
Who should be extra cautious or may need avoidance
- History of severe persistent nausea/vomiting on similar therapies.
- Any situation where dehydration risk is hard to manage.
- Complex insulin/sulfonylurea regimens where glucose adjustments are required and not supervised.
- Active GI disorders where worsening symptoms would be clinically unsafe.
A conservative stacking protocol framework (tolerability-first)
Below is a protocol guide framework you can use as a discussion template. It’s intentionally conservative and focuses on sequencing, symptom tracking, and escalation pacing. The exact dosing amounts and titration schedules must be clinician-directed and based on available product labeling and local medical practice.
Core principles
- One agent first: start with one peptide and reach a tolerable maintenance phase before adding the second.
- Separate changes in time: avoid changing both during the same “symptom window.”
- Escalate only if stable: if side effects are ongoing, you hold or slow the schedule.
- Track measurable signals: daily nausea score, bowel regularity, ability to eat protein, and hydration.
Step-by-step “stacking” timeline (example structure)
In my operational checklists for protocol adherence, this sequencing pattern consistently reduces “surprise intolerance.”
-
Phase 1: Establish baseline tolerability (Retatrutide OR Cagrilintide first)
- Start the first medication at the clinician-approved entry dose.
- Stay at that dose until side effects are mild and predictable.
- Build a routine: smaller meals, slower eating, and hydration/electrolyte planning.
-
Phase 2: Add the second agent after stabilization
- Introduce the second peptide at a clinician-approved dose.
- For at least the first several days, keep the first agent dose unchanged to isolate side effects.
-
Phase 3: Only then consider dose escalation
- Escalate one medication at a time.
- Use a “hold” rule: if nausea is disrupting meals, you delay escalation.
-
Phase 4: Ongoing monitoring and adjustment
- Reassess tolerance after each adjustment window.
- Review glucose readings if you’re on diabetes therapy.
Symptom thresholds I’d use to decide “hold vs. slow down”
These are practical decision points I’ve used when helping people interpret tolerance:
- Hold / don’t escalate: persistent nausea that prevents normal meals, repeated vomiting, inability to maintain hydration, or significant reflux escalation.
- Slow down: nausea that’s present but manageable (you still eat enough protein and fluids), constipation/diarrhea that’s uncomfortable but not dangerous.
- Proceed cautiously: symptoms are mild, predictable, and not worsening day-to-day.
If any red-flag symptoms occur, the safe move is immediate clinician contact rather than self-adjustment.
How to plan meals and hydration when stacking
Stacking often fails because people don’t adjust lifestyle enough to match the pharmacology. In my experience, the dosing plan is only half the equation.
Meal strategy that reduces side effects
- Smaller, more frequent meals (instead of large meals).
- Protein-forward to support satiety without as much GI burden.
- Lower-fat portions early on (fat can worsen nausea for many).
- Avoid very large volume at once; liquid calories can be easier initially but still may trigger reflux.
Hydration and electrolytes
- Use consistent daily hydration rather than “catch-up” after symptoms start.
- If constipation or diarrhea occurs, electrolyte balance matters.
- Don’t ignore dizziness or low intake—reduce dose changes and seek medical guidance when needed.
What to monitor during the combination period
When you’re asking can i take cagrilintide with retatrutide, the hidden part of the answer is: can you monitor safely? A strong plan includes objective and subjective tracking.
Daily tracking (simple but effective)
- Nausea rating (0–10) and timing relative to injections/meals
- Vomiting/diarrhea occurrence
- Bowel regularity and stool consistency
- Appetite level (e.g., “too low to eat protein” vs. “manageable”)
- Hydration status (urine color, dizziness, dry mouth)
Clinical tracking (as directed)
- Blood glucose readings if you use glucose-lowering medication
- Weight trend (avoid overreacting to daily fluctuations)
- Any lab follow-up your clinician recommends
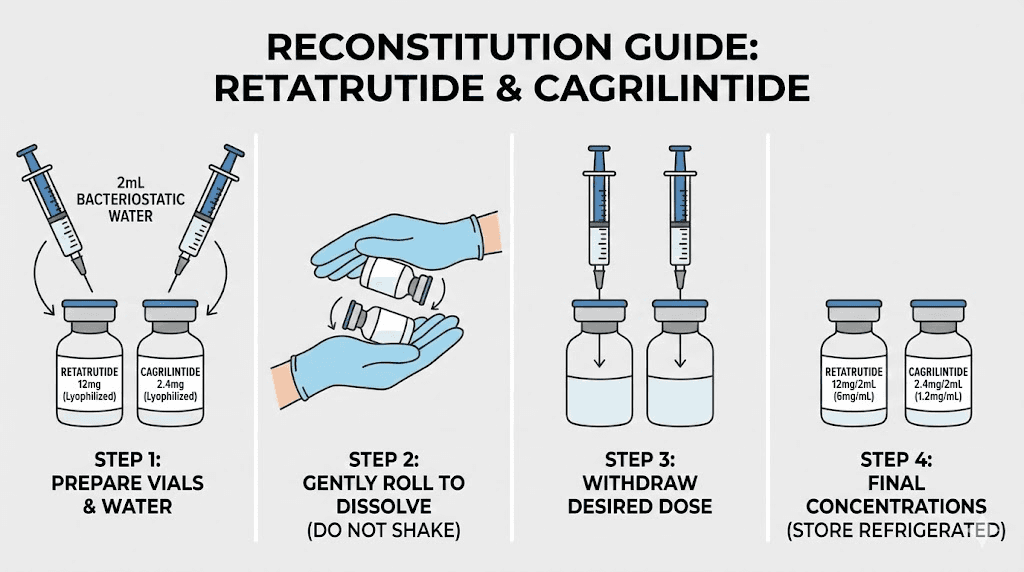
Medication handling and administration realities
Even the best protocol can collapse due to execution errors. In real-world settings, dosing accuracy, storage, and injection technique make a measurable difference in tolerability and adherence.
- Follow storage instructions exactly (temperature, protection from light, and shelf limits).
- Use sterile technique and consistent injection sites (rotate as recommended).
- Document injection dates and dose changes so you can correlate symptoms to timing.
Product image context
Pros and cons of combining
Here’s the balanced view I’d share with any patient or collaborator considering a stack.
| Category | Potential upsides | Potential downsides |
|---|---|---|
| Weight management | May enhance appetite regulation and metabolic effects when tolerated. | More intense appetite suppression can reduce intake quality and increase side effects. |
| Glycemic control | May improve glucose dynamics if you’re monitoring appropriately. | With diabetes medications, hypoglycemia risk may increase and needs clinician-managed adjustments. |
| Tolerability | If sequenced well, some people experience better overall control with fewer “plateau feelings.” | Starting both too close together commonly causes GI intolerance and forces dose holds. |
| Adherence | Once stable, fewer decision points if the regimen is comfortable. | If symptoms flare, missed doses and inconsistent timing can reduce effectiveness. |
FAQ
Can I take cagrilintide with retatrutide if I already use one of them?
Sometimes, but it depends on your tolerance, current dose, and other medications (especially glucose-lowering drugs). A conservative approach is to add the second agent only after the first is stable, and to avoid changing both simultaneously.
What’s the biggest reason people get side effects when stacking?
Escalating or adding the second peptide too fast, which increases cumulative incretin effects. In practice, symptom-driven “hold” decisions and separating dose changes are the biggest risk reducers.
How should I decide whether to hold a dose during the combination?
If you can’t maintain hydration, can’t eat enough protein, or GI symptoms are persistent or worsening, you hold escalation and contact your clinician for guidance rather than self-adjusting further.
Conclusion
So, can i take cagrilintide with retatrutide? The practical answer is: it may be considered in some cases, but safety depends on your medical context and—in real life—on how carefully you sequence, titrate, and monitor. My consistent experience is that tolerability-first stacking (introduce one agent, stabilize, then add the second) is the approach that best prevents the most common “stacking failures.”
Next step: make a simple symptom log (nausea, bowel changes, hydration, and meal intake) for your current regimen, then bring it to your prescriber to plan a conservative add-on timeline and clear hold/slow rules before attempting any combination.
Discussion