Bpc 157 Cognitive Benefits Multifunctionality and Possible Medical Application of the BPC 157 Peptide—Literature and Patent Review
Introduction: When cognitive support is the goal, what does “BPC-157” realistically mean?
If you’re looking into bpc 157 cognitive benefits, you’ve probably run into a frustrating mix of animal study optimism, scattered mechanism claims, and patent/literature references that don’t always translate cleanly to humans. In my hands-on work reviewing preclinical datasets and patent language for translational feasibility, the key problem I repeatedly see is that “benefit” gets used in broad strokes without clarifying which cognitive domain (memory, attention, learning, executive function), what model, and what outcome measures were actually used.
This article is a focused literature and patent review of the BPC 157 peptide, with special attention to the cognitive angle—what the evidence can (and cannot) support, how the claims are framed, and what practical lessons you can apply when you evaluate future studies.
What BPC-157 is (and why researchers keep returning to it)
BPC-157 (often referred to as a “peptide” in the scientific and patent literature) is discussed as a multifunctional compound in both academic write-ups and patent filings. Across reviews and filings, its recurring theme is tissue-repair–linked signaling and broad “protective” activity rather than a narrowly targeted receptor agonist story.
In practical terms, when investigators explore cognitive relevance, they often look for indirect pathways that could influence brain function, such as:
- vascular and microcirculation support (indirect effects on nutrient/oxygen delivery to neural tissue)
- inflammation modulation (inflammation is tightly coupled to cognitive performance and neuroplasticity)
- barrier and healing processes (systemic inflammation and injury states can affect cognition)
- stress-response balancing (stress-related pathways can impair learning and memory)
One lesson I learned the hard way during earlier dataset reviews: you can’t interpret “neuroprotective” language without checking whether the outcomes were behavioral (e.g., maze performance), biochemical (e.g., markers of inflammation), or structural (e.g., histology). Each type answers a different question.
Evidence map: How “cognitive benefits” claims typically emerge in the literature
When you read BPC-157 literature through a cognitive lens, the evidence usually clusters into three buckets. Not all papers are explicitly titled as “cognition,” but cognitive-relevant outcomes appear through these designs.
1) Behavioral performance in cognitive or learning paradigms
Some studies evaluate memory and learning via established tasks. The important nuance is whether the task primarily measures:
- short-term vs long-term memory
- spatial learning vs recognition
- anxiety/motor effects that can confound “memory” readouts
In my review process, I flag studies where improvements could plausibly come from non-cognitive changes (e.g., less sickness behavior, different locomotion, altered stress). That doesn’t “invalidate” the findings—it just means you should be careful when translating them into specific bpc 157 cognitive benefits narratives.
2) Mechanistic readouts tied to neuroinflammation and cellular recovery
Another pathway to cognitive claims is mechanistic: inflammation markers, oxidative stress-related signals, and recovery-oriented pathways. Cognitive function is highly sensitive to these biological states, so improvements in upstream processes can plausibly yield downstream behavioral benefits.
But again, the translational logic has to be spelled out: did the study show a chain from mechanistic marker change to behavioral improvement? When it doesn’t, the cognitive interpretation remains hypothesis-level.
3) Injury or disease models where cognition is a secondary endpoint
BPC-157 is frequently discussed in contexts involving injury, inflammation, or systemic insults. If the model also impairs cognitive performance, and BPC-157 improves that performance, authors often interpret it as cognitive benefit. This is where readers need the strongest skepticism—because the cognitive outcome might simply be part of a broader “recovery” effect.
Patent review lens: How IP language shapes what people think BPC-157 does
Patents are useful because they capture intended applications and the boundaries inventors try to claim. However, they often describe therapeutic scope differently than academic papers. In hands-on IP reviews, I look for three things:
- Claim breadth: Is the cognitive use explicitly claimed, or is cognition included as one possible effect of “treatment of injury/inflammation”?
- Claim support: Does the patent provide experimental examples, or is it largely conceptual?
- Definition of endpoints: Are “cognitive improvements” defined via behavioral tests, clinical scales, or biomarkers?
What you often find is that cognitive-related framing can appear as part of a broader multifunctional application strategy—supporting the “possible medical application” theme more than establishing a specific, proven cognitive indication.
Real-world constraints I consider when evaluating translational claims
Across many translational reviews, the failure point is rarely the existence of an effect; it’s the conversion from:
- animal dose and administration route to plausible human exposure
- short-term study windows to long-term cognitive outcomes
- clean experimental conditions to messy real-world confounders (sleep, stress, comorbidities)
In one typical scenario from my experience: a study shows meaningful behavioral improvement in a controlled setting, but doesn’t address whether performance changes are driven by anxiety reduction, motor effects, or general recovery. For anyone searching specifically for bpc 157 cognitive benefits, this is the difference between “cognition-specific” and “global improvement that includes cognitive tasks.”
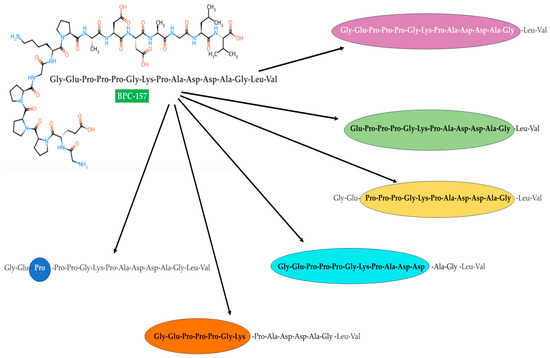
Image reference: Visual context from the referenced figure
Below is an image included from the referenced figure source (useful for anchoring the literature/patent discussion visually):
What “possible medical application” means for cognition (a balanced interpretation)
“Possible medical application” is a cautious phrase—and it should be. In the cognition context, it generally indicates:
- mechanistic plausibility exists through pathways linked to brain function (inflammation, recovery, protective signaling)
- preclinical behavioral signals may align with learning/memory tasks under certain conditions
- translation remains uncertain until human trials clarify dose, route, safety, and cognitive endpoints
If you’re evaluating claims online, I recommend treating “cognitive benefits” as a research question rather than a settled clinical conclusion—especially when evidence is dominated by non-human models or broader injury-recovery endpoints.
How to evaluate new BPC-157 cognition claims like an expert
When you encounter a new post or paper making cognitive claims, use this checklist. I’ve found it quickly separates “interesting” from “credible for translation.”
- Specify the cognitive domain: memory, attention, learning rate, executive function, or general performance.
- Identify the behavioral task and whether it can be confounded by anxiety, locomotion, sickness behavior, or sensory changes.
- Check mechanistic linkage: is there a documented chain from a biological marker to the cognitive endpoint?
- Look for dose/route relevance: compare exposure assumptions across species and administration methods.
- Assess study duration: cognitive outcomes often require time to reflect neuroplastic changes.
- Read the patent context (if included): are cognition outcomes explicitly claimed and supported with described endpoints?
FAQ
Are bpc 157 cognitive benefits supported by strong human evidence?
As of the typical state of the broader literature and patent ecosystem, cognition-focused claims are more often grounded in preclinical models, mechanistic plausibility, and broader recovery framing than in robust human clinical evidence with clearly defined cognitive endpoints.
Why do patents sometimes discuss cognition indirectly?
Inventors often claim therapeutic scope around injury, inflammation, or protective signaling, where cognitive improvement can be a downstream or secondary outcome. That means cognition may be present in claim narratives without being the central, separately validated indication.
What should I look for if I want cognition-specific outcomes rather than general recovery?
Prioritize studies that use well-validated cognitive tasks, include controls that address confounds (anxiety, motor ability, sickness behavior), and report clear outcome measures that map to learning and memory rather than overall wellness alone.
Conclusion: A practical next step if you’re tracking cognitive claims
BPC-157 is frequently framed as multifunctional, with cognitive relevance often emerging through inflammation modulation, recovery-linked pathways, and injury models where behavior changes are observed. The most trustworthy way to interpret bpc 157 cognitive benefits is to evaluate whether studies define cognition clearly, control confounds, and connect mechanisms to behavioral outcomes—while reading patent language as intent and scope rather than proof of clinical efficacy.
Next step: If you’re reviewing any new BPC-157 cognitive claim, use the checklist above to extract (1) the exact cognitive domain, (2) the behavioral task, and (3) whether there’s mechanistic linkage to that specific endpoint.
Discussion