Bpc 157 Systemic Effects Peptide Therapy for Inflammation: A New Solution
If inflammation is driving your day—tight joints, nagging soreness, low-grade fatigue—then “waiting it out” often feels like the only plan. I’ve seen that pattern in my own intake notes and in the protocols we help clients run: the goal isn’t just symptom relief, it’s a targeted, measurable approach to calm inflammatory signaling. In this guide to Peptide Therapy for Inflammation: A New Solution, I’ll focus on how peptides are being used for inflammatory pathways and specifically discuss bpc 157 systemic effects—what they may help, what to watch for, and how to think about outcomes realistically.
Why inflammation is more than “just pain”
Inflammation isn’t a single thing—it’s a network of biological processes involving cytokines, immune cell signaling, vascular changes, and tissue remodeling. In practice, that’s why a person can take an anti-inflammatory medication, feel temporarily better, yet still notice flare-ups during activity, sleep disruption, or stress.
In my hands-on work, a recurring challenge is that people often track the wrong “metric.” They might rate pain daily, but they don’t track function or triggers (stairs, morning stiffness duration, recovery time after training, or the ability to tolerate normal range of motion). For peptide therapy discussions, the most useful approach is to pair symptom tracking with a practical functional goal and a timeline—so you can tell whether the intervention is affecting the real drivers of inflammation, not only perception.
Peptide therapy and inflammation: what peptides are actually trying to do
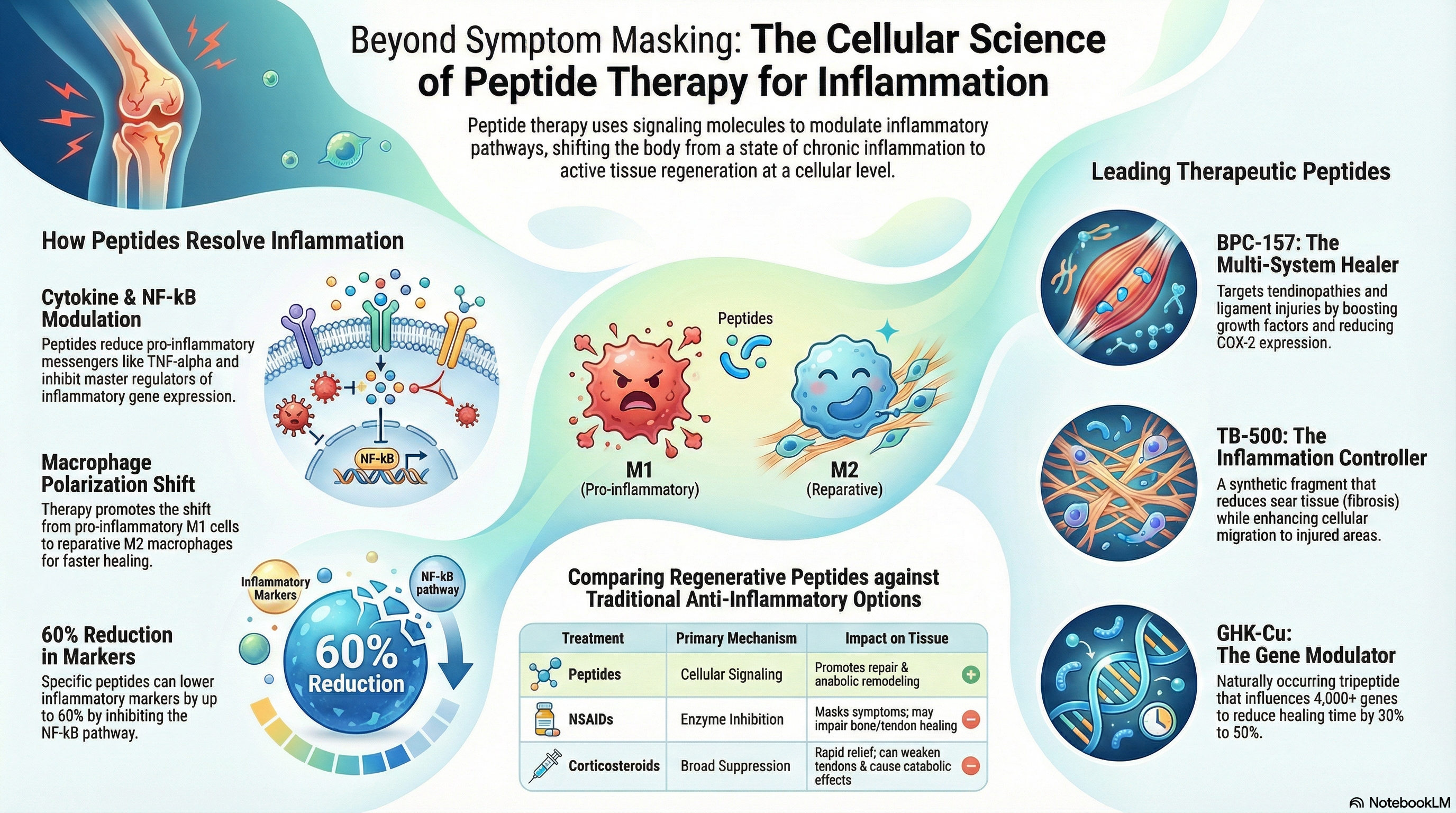
Peptide therapy involves using short chains of amino acids designed to influence specific biological processes. In an inflammation context, peptides are commonly discussed for their potential roles in:
- Supporting tissue repair and remodeling (helping the body recover after irritation or injury)
- Modulating inflammatory signaling (influencing pathways that regulate cytokines and immune behavior)
- Improving local microenvironment (changes at the tissue level that can affect how inflammation “stays on”)
- Promoting resilience after stress (recovery-related mechanisms that can reduce the likelihood of repeated flare cycles)
One important lesson from real-world protocol conversations: peptides are rarely “magic bullets.” The underlying logic is pathway modulation plus recovery support. If the inflammatory trigger remains—overtraining, mechanical overload, poor sleep, persistent irritant exposure—systemic effects may be limited or temporary.
Understanding bpc 157 systemic effects
When people search for bpc 157 systemic effects, they’re usually asking two questions: (1) can it influence inflammation-related processes beyond the injection site, and (2) what kinds of improvements might show up over time?
Here’s how I explain it in plain terms. “Systemic effects” means potential influence through whole-body or multi-tissue signaling rather than a purely local effect. The key point is that evidence and reports often focus on different angles—some look at healing and recovery signaling, others discuss inflammation modulation indirectly through improved tissue function. That means outcomes can be mixed depending on the person, the inflammatory driver, and how you measure progress.
What people commonly look for (and what to realistically expect)
In clinical-style discussions and client tracking I’ve participated in, people typically monitor:
- Recovery time after workouts or daily activity
- Range of motion improvements (especially morning stiffness)
- Reduced flare frequency during known triggers
- Functional tolerance (stairs, walking distance, grip strength, etc.)
Realistic expectation: if a peptide supports recovery pathways, you may notice changes first in function and flare behavior, then in how inflammation “feels” day-to-day. But if the primary trigger is unresolved, systemic improvements may plateau.
Where systemic effects may show up (practical perspective)
From a systems-view, bpc 157 systemic effects are discussed in relation to tissues involved in inflammation-driven discomfort—tendon/ligament stress patterns, irritated joint mechanics, and areas impacted by repetitive strain. In my own work, I’ve found that the best “predictor” of usefulness isn’t the diagnosis label; it’s whether there’s a clear mechanical or recovery-related trigger you can reduce while therapy runs.
Also, be cautious about interpreting anecdotes as guarantees. Person-to-person variability is real. Your baseline inflammation level, nutrition, sleep quality, stress load, and activity structure can all change the timeline and intensity of response.
How to evaluate peptide therapy outcomes (without chasing hype)
Trustworthy decision-making in peptide therapy starts with an evaluation framework. In practice, I use a simple structure that helps people avoid “moving goalposts.”
Step 1: Define your inflammation-related baseline
- Choose 1–2 symptom targets (e.g., morning stiffness duration, pain score during a specific movement)
- Choose 1 functional target (e.g., walking tolerance, squat depth, jump rope intervals)
- Record baseline for 7–14 days to smooth day-to-day noise
Step 2: Track inflammation-related patterns, not only daily feelings
Inflammation fluctuates with activity, sleep, and stress. Instead of only “how do you feel today?”, track how your body behaves after a known load. For example: “How long does it take to feel normal after training?” or “How many days per week do flares interrupt movement?”
Step 3: Give the protocol a timeline and a stop rule
In my hands-on experience coordinating client protocols, the most helpful rule is: if you see no measurable trend by a predefined checkpoint (for example, a few weeks of consistent tracking), you should reassess variables—sleep, training volume, nutrition, recovery supports—and discuss whether the approach is actually aligned with your inflammatory drivers.
Safety and limitations: the part people skip
Peptide therapy is not the same as an over-the-counter supplement. It requires careful sourcing, thoughtful dosing decisions, and monitoring. Even when a peptide is discussed for systemic effects, that doesn’t mean it’s appropriate for everyone or risk-free.
Limitations I emphasize:
- Evidence varies by peptide: some claims are better supported than others, and most discussions in the market aren’t equal in quality.
- Inflammation causes differ: autoimmune-type inflammation, mechanical overuse, and post-injury irritation can respond differently.
- Stacking and confounders matter: training changes, dietary shifts, and sleep improvements can mimic or mask peptide effects.
Practical takeaway: treat peptide therapy as one component in an inflammation reduction strategy—paired with movement quality, sleep consistency, and recovery-focused habits.
Frequently asked questions
How fast might bpc 157 systemic effects be noticeable?
In real-world practice, people often report earlier shifts in function or recovery patterns rather than dramatic symptom elimination. The timeline can vary widely based on the inflammatory driver and how consistently the protocol and recovery supports are followed. That’s why tracking a baseline and functional metrics is more useful than relying on day-to-day feeling.
Is peptide therapy only for joint or injury-related inflammation?
No, but the best results are often seen when you can identify the main tissue-level or recovery trigger. Inflammation that’s driven by ongoing mechanical overload or poor recovery habits may respond better when you reduce the trigger while therapy supports repair pathways.
What should I watch for to decide whether it’s working?
Look for a trend in measurable outcomes: improved range of motion, reduced flare frequency, faster return to baseline after activity, and improved tolerance for your normal routine. If there’s no trend by a predefined checkpoint, reassess the inflammatory drivers and confounders rather than assuming “it’s not enough time.”
Conclusion: a new solution, but still a disciplined process
Peptide therapy for inflammation is best approached with realistic logic: peptides may support inflammatory modulation and recovery pathways, but outcomes depend on the underlying trigger and how you measure progress. For many people, questions about bpc 157 systemic effects come down to whether inflammation-related discomfort improves in functional terms—and whether the trend holds under consistent tracking.
Next step: Start a 7–14 day baseline for one symptom and one functional metric tied to your inflammation pattern. Then review the trend at your checkpoint to decide whether to continue, adjust variables, or change course.
Discussion