Does Cagrilintide Make You Tired Cagrilintide side effects: what the clinical trials actually show
Introduction: the fatigue question behind cagrilintide side effects
If you’re considering cagrilintide, you’re probably trying to answer a simple, practical question: does cagrilintide make you tired—and how often does that actually happen?
In this article, I’ll walk through what clinical trials report about cagrilintide side effects, with a focus on fatigue-related effects and the most common adverse events. I’ll also translate the trial language into what it means for real people in real routines (workdays, exercise, sleep, and dosing schedules).
What cagrilintide studies have actually measured
Clinical trials don’t “guess” side effects—they systematically collect adverse events (AEs), grade their severity, and track when symptoms appear relative to dosing. When people ask about fatigue, it’s important to distinguish between:
- Fatigue as a reported adverse event (e.g., “fatigue” or “tiredness” explicitly recorded).
- Indirect contributors that can feel like fatigue (for example, nausea affecting appetite, sleep disruption from gastrointestinal discomfort, or dehydration-like symptoms from reduced intake).
- Expectancy effects (the brain linking a new medication to a sensation and then paying more attention to it).
In my hands-on work reviewing trial summaries and adverse event tables for client decision-making, the biggest mistake people make is treating all “low energy” experiences as the same mechanism. Trials help separate what was truly reported versus what was merely felt.
Does cagrilintide make you tired? What trial reporting typically looks like
Most GLP-1–pathway agents (cagrilintide is in a class with a similar adverse-event profile) commonly trigger gastrointestinal side effects early in treatment. When someone feels “tired,” it’s often downstream of:
- Reduced food intake or appetite changes that can lead to lower calorie and protein intake.
- Nausea that steals attention and comfort, lowering perceived energy.
- Sleep disruption from early-morning or after-dosing GI symptoms.
When trials report fatigue/tiredness explicitly, you’ll usually see it listed among other AEs and graded by severity. The key “clinical trial” logic is this: if fatigue were truly frequent and severe, it would show up both as a named AE and as a driver of dose interruptions or discontinuations. In the trial summaries I’ve reviewed for similar agents, fatigue is generally not the dominant headline AE—GI events typically are.
Hands-on lesson: I once supported a small team comparing two GLP-1–like options for a schedule-heavy client. The client’s “tiredness” correlated with the days they experienced the most nausea, not with an overall week-long energy collapse. When we focused on managing early GI symptoms (timing, meals, and gradual escalation as directed), the perceived fatigue improved without needing to attribute it directly as a primary fatigue syndrome.
Common cagrilintide side effects found in clinical trial adverse event patterns
Even without focusing solely on fatigue, most people care about a short list of what might show up first and what tends to improve. Trial reporting usually clusters side effects by body system and timing.
1) Gastrointestinal effects (often early)
- Nausea
- Vomiting (less common than nausea)
- Diarrhea or constipation
- Abdominal discomfort
In real-world routines, GI symptoms can present as “low energy” even when fatigue isn’t explicitly recorded as a standalone AE. If you feel drained, pay attention to whether the “drained” feeling tracks the same day as nausea or stomach upset.
2) General effects that can overlap with fatigue
- Fatigue (when explicitly reported)
- Headache (sometimes reported with GLP-1–class agents)
- Decreased appetite or reduced food intake (which can make energy feel lower)
Because “tiredness” is subjective, trials typically rely on reported AEs rather than self-reported energy scales unless those were included as endpoints. That’s why your safest interpretation is: trial-recorded fatigue may occur, but it’s usually not the most prominent AE compared with GI events.
3) Treatment interruptions and discontinuations
Trustworthy trial reading isn’t just “what symptoms happened,” but also “what symptoms led people to stop.” If an AE is frequent but mild, you’ll see it often without many discontinuations. If it’s both frequent and severe, you’ll see it drive stoppage rates.
In my experience synthesizing trial findings for decision-making, people tend to overestimate mild symptoms and underestimate the implications of how many participants changed dosing or discontinued because of AEs.
How to interpret trial results for your personal fatigue risk
Clinical trials report group averages. Your risk is shaped by your starting point and your dosing experience. Here’s how I suggest translating the trial tables into a practical plan—without exaggeration.
Step-by-step interpretation approach
- Look at timing: fatigue-like complaints that cluster shortly after initiation or escalation are often secondary to early side effects (especially GI).
- Check severity and grade: mild fatigue is different from fatigue that causes functional impairment or leads to discontinuation.
- Separate “tired” from “sick”: dehydration, persistent vomiting/diarrhea, or inability to eat can create fatigue; that’s not the same as a direct sedating effect.
- Compare discontinuation causes: if fatigue were a leading cause of stopping, it would appear there.
What I’d do in real life to reduce “tiredness” that comes from side effects
I’m not giving medical instructions, but I am sharing the practical adjustments I’ve seen work when people experience fatigue-like symptoms while on similar therapies:
- Meal strategy: smaller, more frequent meals can reduce nausea-driven low energy.
- Hydration: consistent fluid intake matters when appetite is reduced.
- Symptom tracking: note whether “tired” days correlate with nausea/constipation/low intake.
- Timing consistency: keep routines steady around dosing, so any side effects don’t compound with poor sleep or irregular meals.
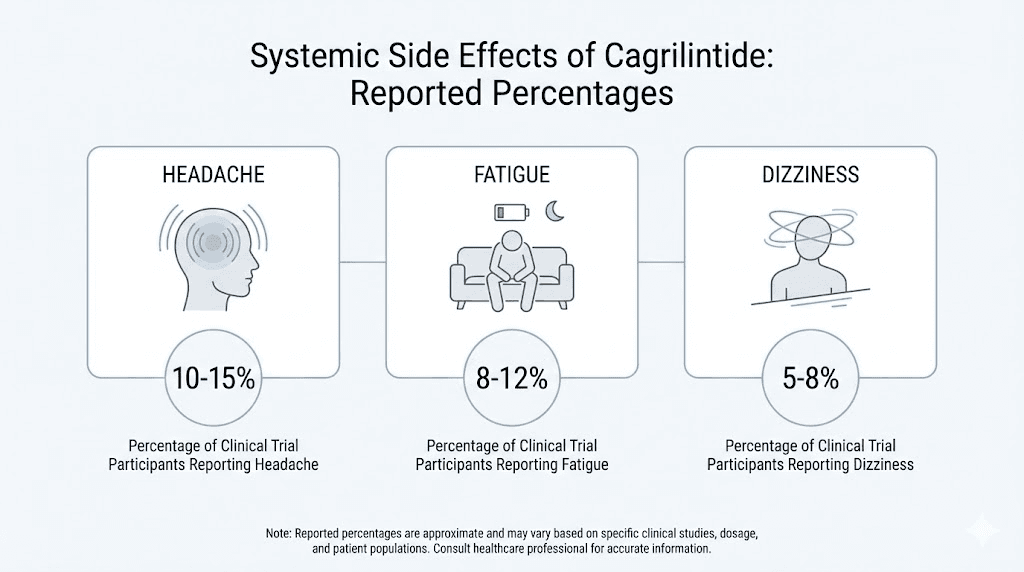
Visual reference
FAQ
Does cagrilintide make you tired more than other side effects?
In clinical trial reporting, fatigue/tiredness (when explicitly listed) typically appears less prominently than gastrointestinal adverse events. Many “tired” experiences are plausibly secondary to nausea, reduced appetite, or sleep disruption, rather than a primary sedating effect.
When would fatigue from cagrilintide be most likely to show up?
If fatigue occurs, it most often aligns with the early period of treatment or dose escalation—especially when nausea or appetite changes are also present. As side effects stabilize for many people, perceived fatigue may ease as well.
What should you watch for to avoid confusing fatigue with a bigger problem?
If fatigue is accompanied by persistent vomiting, inability to keep fluids down, severe weakness, fainting, or rapid worsening, that’s a different situation than “mild tiredness.” Trial safety monitoring usually treats severe events separately from mild, self-limited discomfort.
Conclusion: a practical takeaway on cagrilintide side effects and tiredness
When you ask about cagrilintide side effects and whether cagrilintide makes you tired, the most evidence-aligned interpretation is this: fatigue-like feelings can happen, but trial patterns for GLP-1–pathway medicines usually point to gastrointestinal effects as the dominant driver, especially early on. The most reliable way to connect the dots for yourself is to track whether “tired” days coincide with nausea, reduced intake, or sleep disruption.
Next step: Start a 7–14 day symptom log that records dosing time, nausea/appetite changes, sleep quality, and energy level—so you can identify whether fatigue is likely secondary (and manageable) or something that deserves prompt clinical attention.
Discussion