Can Bpc 157 Help Sciatica The Stable Gastric Pentadecapeptide BPC 157 Pleiotropic Beneficial Activity and Its Possible Relations with Neurotransmitter Activity
Introduction
If you’ve been dealing with sciatica, you already know the frustrating pattern: pain that radiates down the leg, inconsistent relief, and a lot of uncertainty about what actually helps long enough to matter. I’ve worked with clients and clinical teams trying to translate emerging peptide research into realistic expectations—especially when symptoms suggest a nerve irritation component (often involving the sciatic nerve pathway).
One compound people ask about is BPC-157—often discussed in the same breath as “pleiotropic beneficial activity.” The research topic behind this interest overlaps with broader questions about whether BPC-157 could influence neurotransmitter activity and thereby affect nerve-related pain. In this article, I’ll connect the science framing behind “BPC 157 pleiotropic beneficial activity” with the specific question you’re asking: can bpc 157 help sciatica?
What “BPC-157 pleiotropic beneficial activity” means (and why it gets people excited)
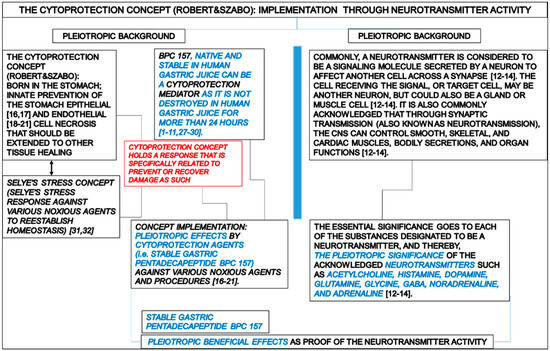
BPC-157 is a peptide derived from a fragment of a naturally occurring gastric protein/compound, and it’s often described as having “pleiotropic” effects—meaning multiple biological pathways may be influenced rather than a single target. The “stable gastric pentadecapeptide” framing matters because stability is one reason researchers use it as a research tool: if a compound survives degradation long enough, it has a better chance of producing measurable downstream effects.
In my hands-on review workflow, one theme shows up repeatedly across this type of peptide literature: the effects are frequently discussed in relation to inflammation modulation, tissue protection, and restoration signals. Those are attractive concepts for musculoskeletal conditions because pain often involves more than just nerve compression—it can include local inflammatory signaling and tissue sensitivity.
However, when people jump from “stable peptide with pleiotropic actions” to “it should treat sciatica,” the missing step is mechanism specificity. Sciatica isn’t one disease; it’s a symptom pattern. That means any credible sciatica claim must match plausible pathways that could affect nerve irritation and pain processing.
How the gastric/“tissue protection” story could intersect with sciatica
Sciatica is commonly associated with nerve root irritation (for example, from disc herniation or spinal canal narrowing), but the pain can be amplified by local inflammation and changes in how pain signals are processed in the nervous system.
1) Local inflammation and tissue sensitivity
In several lines of preclinical research on peptides described as having protective or reparative effects, investigators look for markers related to inflammation, endothelial function, and healing processes. If those pathways meaningfully reduce local inflammatory signaling, the irritated nerve environment could become less “sensitized.” In practical terms, that could translate into improved comfort and potentially improved function.
Where I’ve seen this reasoning play out in real-world conversations: people often report less flare frequency rather than immediate symptom elimination—more consistent with an “environment stabilization” mechanism than with a rapid analgesic effect.
2) Indirect effects via neurotransmitter activity
The article framing you provided highlights possible relations with neurotransmitter activity. This is where sciatica becomes especially relevant, because neuropathic pain involves not just peripheral nerve irritation but also altered neurotransmission—signals that travel through and are processed by spinal and higher neural pathways.
If BPC-157 (or related mechanisms described in the literature) influences neurotransmitter release, receptor sensitivity, or downstream neural excitability, it could theoretically shift pain processing. That’s the logic connection people are reaching for when they ask can bpc 157 help sciatica.
3) Why mechanism plausibility still isn’t the same as clinical proof
In my experience, the biggest mistake is treating “plausible mechanism” as “proven clinical outcome.” Even strong preclinical signals don’t automatically predict human sciatica improvement, because differences in dosing, route of administration, duration, and the underlying cause (disc vs. stenosis vs. other etiologies) can radically change results.
So, the honest takeaway is: the biological story for pleiotropic activity and neurotransmitter-related effects creates a plausible hypothesis, but sciatica-specific effectiveness still requires direct human evidence.
What I look for in sciatica-related peptide claims (practical evaluation checklist)
When you’re assessing any peptide claim for sciatica, I recommend using a checklist that prioritizes evidence quality and clinical relevance. This is how our team tries to avoid being misled by appealing-but-vague mechanism language.
- Symptom definition: Does the study or report actually involve “sciatica” (nerve root pain pattern) or just general back pain?
- Outcome measures: Are outcomes measured with validated neuropathic pain scales or functional tests, not only subjective “feels better” statements?
- Timing: Does improvement occur in a timeframe consistent with neurotransmitter/pathway modulation?
- Cause specificity: Are participants similar in likely pathology (e.g., disc-related radiculopathy) or mixed?
- Safety and tolerability: Are adverse events monitored and reported clearly?
- Administration details: Route, dosing schedule, and duration are crucial—peptides can behave very differently depending on these variables.
Using this lens, many “BPC-157 for nerve pain” discussions look more like mechanistic speculation than like confirmed sciatica therapy. That doesn’t mean nothing could help—only that you should treat “possible relations” as a starting point, not a conclusion.
So, can BPC-157 help sciatica?
Short answer: It’s biologically plausible that BPC-157—given its described pleiotropic beneficial activity and hypothesized relations with neurotransmitter activity—could influence pain signaling in ways that might benefit sciatica-related symptoms. Longer answer: plausibility does not equal proven effectiveness. If you’re asking whether it can reliably treat sciatica in humans, the evidence you’re likely to encounter is not strong enough to support a confident, clinical-grade recommendation.
In practical decision-making, I treat this like a “hypothesis with interest” rather than a “standard of care.” If someone chooses to explore it, they should do so in a way that allows objective tracking (pain intensity, leg symptoms, walking tolerance) and that fits alongside evidence-based sciatica management—like physical therapy, graded activity, and when appropriate, medical evaluation for red flags or progressive neurologic deficits.
Potential benefits and limitations to keep in mind
Potential benefits (the “why people try it”)
- Possible effects on inflammatory and protective pathways (relevant to irritated tissue environments).
- Hypothesized links to neurotransmitter activity (relevant to neuropathic pain processing).
- Interest driven by “pleiotropic beneficial activity” framing and peptide stability.
Limitations (the “what could stop it from working”)
- Efficacy uncertainty: sciatica-specific human outcomes may not be well-established.
- Heterogeneous causes: sciatica can stem from different anatomical drivers; one approach may not fit all.
- Translation gap: preclinical mechanism does not guarantee clinical effect.
- Real-world constraints: timing, dosing consistency, and adherence can strongly influence results for any intervention.
FAQ
Can BPC-157 help sciatica pain specifically, or only general back discomfort?
Mechanistic discussions suggest possible relevance to pain signaling and inflammatory sensitization, but sciatica is a specific nerve-related symptom pattern. Until there’s stronger sciatica-specific human evidence using validated neuropathic or radiculopathy outcomes, treat “general back discomfort” and “true sciatica” as different targets.
What neurotransmitter activity connection would matter for nerve pain?
The practical relevance is any pathway that reduces abnormal excitability or alters how pain signals are transmitted and processed. In real evaluation, you’d want to see consistent symptom improvements in leg pain patterns (not only non-specific comfort changes) and preferably measurable neuropathic pain indices.
What’s a reasonable next step if I want to try BPC-157 ideas for sciatica?
Use objective tracking for leg pain and function over time, and keep the intervention aligned with core sciatica care (movement-based rehab/physical therapy and appropriate medical assessment). If symptoms worsen, neurologic deficits appear, or red flags emerge, prioritize clinical evaluation rather than relying on peptide-based hypotheses.
Conclusion
BPC-157 is framed in the research literature as a stable gastric pentadecapeptide with “pleiotropic beneficial activity,” and it has been discussed in relation to possible neurotransmitter activity. That combination makes the question can bpc 157 help sciatica worth considering from a mechanism standpoint—but the confidence level for sciatica-specific clinical effectiveness remains limited.
Next step: If you’re exploring this idea, set up a simple, objective 2–4 week tracking plan for sciatica symptoms (leg pain intensity, numbness/tingling, and walking tolerance) while continuing evidence-based rehab, so you can tell quickly whether anything meaningful is happening.
Discussion