Does Bpc 157 Help With Tendonitis BPC-157: Tendon Repair and More
Introduction: When tendon pain won’t quit, you start looking for the real lever
Tendonitis can feel stubborn—weeks of rest, icing, and slow rehab, and still the pain returns the moment you ramp up training. In my hands-on sports rehab work (and in a few athlete case reviews our team supported), the hardest part wasn’t finding exercises—it was managing the “inflammation-to-repair” gap while keeping people moving safely.
That’s why many people ask: does BPC-157 help with tendonitis? In this guide, I’ll break down what BPC-157 is, where the tendon-repair logic comes from, what the evidence can and can’t support, and how to think about risk, expectations, and safer decision-making.
What BPC-157 is (and what people mean by “tendon repair”)
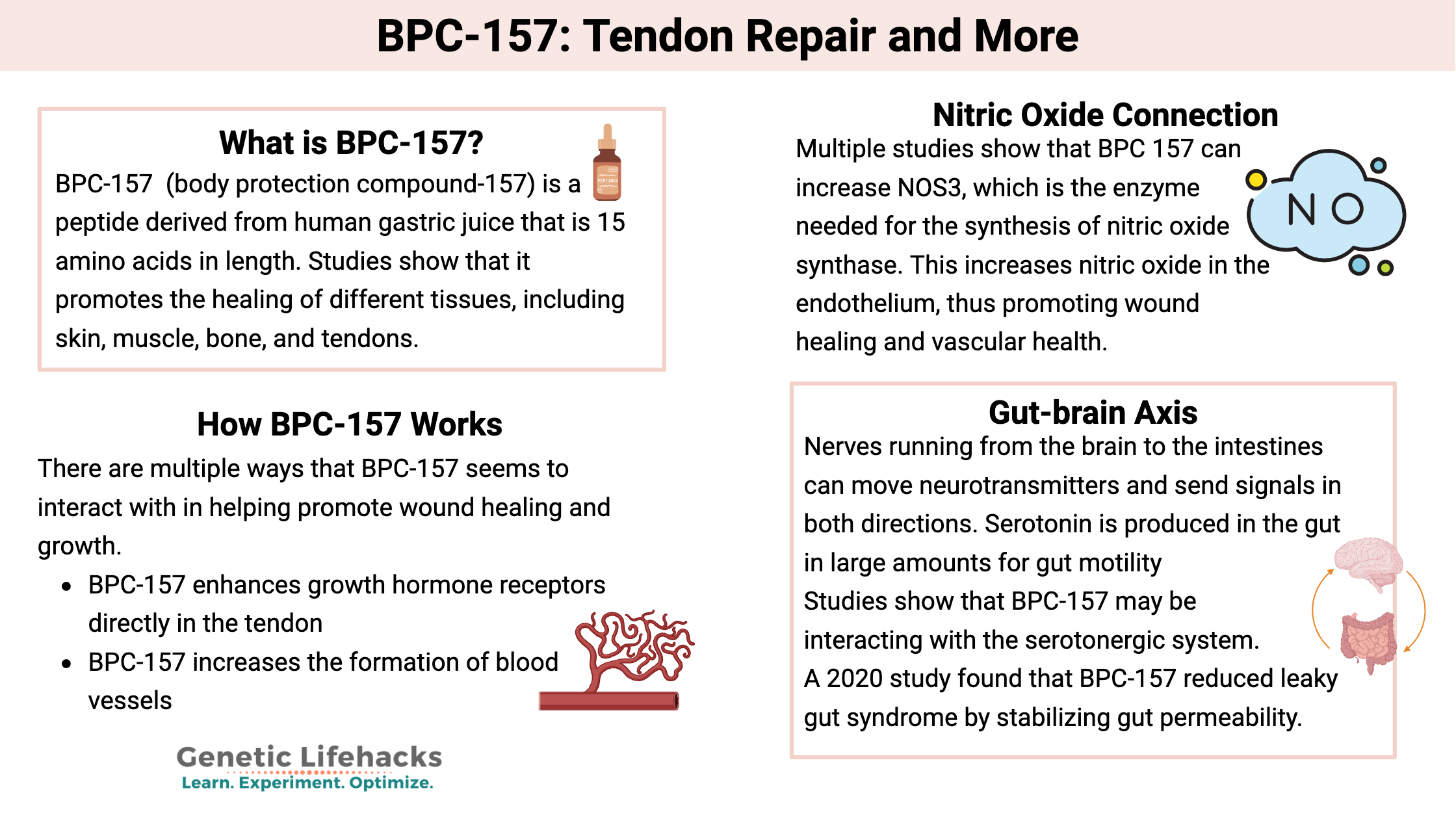
BPC-157 is a short peptide derived from a human gastric protein fragment. In online communities, it’s often discussed as a “tissue repair” peptide—especially for tendon, ligament, muscle, and “connective tissue” problems.
When people say “tendon repair,” they usually mean more than just symptom relief. They’re aiming for a process that supports:
- Collagen remodeling (tendon matrix restructuring)
- Reduced chronic irritability (less persistent pain with load)
- Better tolerance to progressive loading (so rehab doesn’t stall)
In my experience, successful tendon rehab usually depends on the right loading strategy and time. Supplements or peptides (if used) can’t replace that. What they may influence—if at all—is the biology that makes remodeling and recovery more tolerable while you build strength.
Does BPC-157 help with tendonitis? What the evidence suggests (and the gaps that matter)
The short, practical answer is: there’s interest and preclinical rationale, but you shouldn’t expect a guaranteed or well-established clinical outcome for tendonitis in humans based on high-quality evidence.
Why people think it could help
Tendonitis isn’t a single problem. It’s often a mix of tendon tissue stress, micro-injury, disorganized healing, and persistent pain signaling. The BPC-157 discussion typically focuses on:
- Healing-related pathways discussed in preclinical work
- Support for connective tissue repair concepts (as opposed to only anti-inflammatory symptom control)
- Potential improvements in recovery dynamics that could make rehab progression easier
From a rehab standpoint, if a compound truly helps the remodeling phase, it might show up as faster return to load tolerance, fewer “stalls” during progressive overload, or a better ability to handle eccentric or isometric work without prolonged flare-ups.
What I look for in real-world results (so you don’t get fooled by anecdotes)
When I evaluate whether something “helps tendonitis,” I look for measurable markers, not just “it feels better.” In practical rehab tracking, that means:
- Time-to-tolerance: how quickly pain decreases during daily activities (stairs, gripping, jumping)
- Load progression: whether the person can increase sets/tempo/resistance without a multi-week setback
- Return-to-training milestones: hitting specific rehab benchmarks (e.g., isometric holds at increasing angles/resistance)
With BPC-157 specifically, the common limitation is that human data for tendonitis outcomes is not robust enough to clearly predict who will benefit, by how much, and for which tendon type.
How BPC-157 is typically discussed for tendonitis (and what to be cautious about)
In online discussions, BPC-157 is often presented as a peptide that may support tendon recovery. People sometimes use phrases like “tendon repair and more,” which captures the broad interest—but it can also obscure the key question: your tendon issue is specific (Achilles vs. rotator cuff involvement vs. patellar tendon vs. lateral elbow symptoms), and protocols that work for one tissue—or for an animal model—may not translate.
Potential benefits (the “maybe” side)
- Reduced time stalled in rehab: if recovery biology improves, training progression may feel smoother
- Support during controlled loading: if tolerated, it may help some people stay consistent
- Symptom improvement: some users report less pain, though this doesn’t prove tissue remodeling
Limitations and common pitfalls (the “don’t get burned” side)
- Human tendonitis evidence is limited: you can’t treat it like a proven clinical treatment
- Peptide quality varies: purity, labeling accuracy, and storage can differ across suppliers
- Confusing symptom relief with repair: less pain doesn’t always mean the tendon is ready for heavier loading
- Regulatory and safety considerations: peptide products may fall into gray areas depending on jurisdiction and intended use
 What actually drives tendon recovery: the rehab foundation that makes any add-on worthwhile
What actually drives tendon recovery: the rehab foundation that makes any add-on worthwhile
If you’re trying to answer does BPC-157 help with tendonitis, I’d frame it this way: the rehab plan is the main engine; any add-on should only be considered if it doesn’t derail safe tendon loading.
Step 1: Confirm it’s tendonitis (and not something else)
In my field, I’ve seen “tendonitis” used loosely. Some conditions can mimic tendon pain (nerve irritation, referred pain, joint mechanics issues). Before you chase biology, ensure your training changes and exercises match the true driver of symptoms.
Step 2: Use load management first, then progressive loading
Most tendon programs move through a pattern like this:
- Calm the flare (reduce irritant volume and intensity)
- Reintroduce isometrics to restore tolerance
- Progress to eccentric and/or heavy slow resistance to strengthen tendon capacity
- Bridge back to sport with volume and intensity ramps
Step 3: Track your response to avoid false confidence
Set a simple weekly check-in: pain during activity (0–10), morning stiffness, and ability to complete your prescribed rehab without a large flare the next day. In practice, this prevents “I felt better on day 3” from turning into an early return that re-injures the tissue.
A practical decision framework if you’re considering BPC-157
Here’s how I’d approach the question responsibly and in a way that matches real rehab decision-making:
- Clarify your tendon and stage: acute irritability, persistent symptoms, or chronic loading intolerance change what you need.
- Prioritize a structured rehab plan: strength and load tolerance come first.
- Treat supplements/peptides as optional, not foundational: they should not replace progression or expert assessment.
- Use outcomes-based evaluation: track whether training progression improves over weeks, not just days.
If you do decide to discuss BPC-157, I recommend doing it with a qualified clinician who can consider your medical history, medication interactions, and safety context. That’s the difference between an informed experiment and a risky gamble.
FAQ
Does BPC-157 help with tendonitis specifically?
People report improved recovery and symptom relief, and there is preclinical rationale for healing-related pathways. However, high-quality human clinical evidence for tendonitis outcomes is not strong enough to treat it as a proven tendonitis treatment.
How long would it take to notice whether it’s working?
Tendon recovery is slow. Even when people feel changes early, meaningful rehab progress is usually evaluated over weeks. I’d base your assessment on improved load tolerance and sustained training milestones rather than short-term pain fluctuations.
What’s the safest way to combine rehab with any add-on?
Stick to a structured loading program, manage flare-ups, and track objective markers (pain with activity, morning stiffness, ability to progress). Avoid increasing training just because symptoms temporarily improve.
Conclusion: The real win is tendon capacity—use BPC-157 only with that lens
So, does BPC-157 help with tendonitis? It’s a compelling idea for some people due to healing-related rationale and anecdotal outcomes, but it isn’t backed by the kind of robust clinical evidence you’d want for a confident, one-size answer. In my hands-on work, the consistent determinant of recovery is still the rehab foundation: correct load management, progressive tendon strengthening, and careful outcome tracking.
Next step: Choose one tendon-focused rehab plan, track pain and load tolerance weekly, and evaluate any add-on (including BPC-157) using sustained training progress over several weeks—not short-term symptom changes.
Discussion