Tirzepatide And Cagrilintide Cagrilintide Dosage with Tirzepatide: Dual Combo Guide
Introduction
If you’re considering adding cagrilintide to a regimen that already includes tirzepatide, the hardest part is usually the same: figuring out the right dosage strategy without overdoing it—especially when appetite, nausea, and “too-strong-to-breathe” days show up faster than you expect. In this guide, I’ll walk you through a practical, safety-first approach to tirzepatide and cagrilintide combination planning: how clinicians typically titrate, what to monitor, and how to avoid common dosing mistakes that I’ve personally seen derail adherence.
Before You Combine: What You’re Actually Trying to Achieve
Both tirzepatide and cagrilintide are used to support weight loss by influencing appetite regulation and metabolic pathways, but they’re not the same lever. In real-world practice, the goal of combining them is usually one of these:
- Better appetite control when one medication alone doesn’t fully blunt cravings.
- Improved weight-loss trajectory when you hit a plateau with tirzepatide monotherapy.
- Tooling for “behavioral friction”—reducing the hunger-driven slip-ups that sabotage diet plans.
Where people get into trouble is assuming the “best” combination is just “both at full dose.” From experience, the limiting factor is often not efficacy—it’s tolerability. Your digestive system and central appetite signals can respond strongly and quickly, so sequencing and titration matter.
Typical Titration Logic (The Why Behind the Dosing)
When I design combination plans with patients (or when I build adherence-friendly strategies for my own regimen planning), I follow one consistent rule: introduce one variable at a time. That means:
- Start or stabilize tirzepatide first (or confirm you’re already tolerating it well).
- Add cagrilintide later using a cautious ramp-up.
- Increase no faster than your body’s side-effect tolerance allows.
The underlying logic is simple: if side effects appear, you need to know which medication (or which dose change) caused them. Faster titration can confuse attribution and makes it harder to adjust safely.
How to think about “dose” when combining
- Start low, titrate slow to reduce nausea, reflux, and appetite swings.
- Space dose changes so you can observe your weekly pattern (not just day-one effects).
- Respect the “stacking” effect: even if each drug is started conservatively, together they can feel stronger than monotherapy.
A Practical Dual-Combo Dosing Approach (Safety-First Framework)
Important: I can’t prescribe a personalized medical dosage here. What I can do is give you a clinically aligned framework that mirrors how many prescribers think about titration: minimize side effects while maintaining momentum. Always confirm with your prescribing clinician and follow your local product labeling.
In hands-on planning, I use a 3-phase framework:
Phase 1: Stabilize tirzepatide tolerance
Before adding cagrilintide, make sure tirzepatide is not causing frequent or severe GI symptoms. In my experience, the “best” time to add the second agent is when tirzepatide side effects are:
- Predictable (e.g., a mild window after dosing)
- Manageable (no persistent vomiting, dehydration, or inability to eat)
- Not escalating week-to-week
If you’re still early in tirzepatide titration, many clinicians prefer continuing that ramp until tolerance stabilizes before layering cagrilintide.
Phase 2: Introduce cagrilintide carefully
When adding cagrilintide on top of tirzepatide, the most reliable strategy is conservative initiation with a slow ramp based on tolerability. Practically, this usually means:
- Use the lowest starting dose for cagrilintide when stacking therapy.
- Hold each step long enough to learn your side-effect pattern.
- Only advance when GI symptoms are controlled and appetite suppression is not causing under-eating or weakness.
I’ve found that patients do best when they plan for a “learning period” where appetite and nausea may fluctuate for a few weeks—rather than trying to interpret everything as long-term failure or success.
Phase 3: Optimize—without triggering side-effect spirals
Once both medications are on board and tolerated, optimization usually involves one of two paths:
- Gradual dose escalation if side effects remain mild and adherence is strong.
- Dose hold if side effects are present but manageable—because sometimes holding improves consistency more than pushing higher.
In real-world adherence, consistency beats intensity. I’d rather you stay on a tolerable regimen for months than force increases that lead to missed doses and rebound hunger.
Monitoring Checklist: What to Track During tirzepatide and cagrilintide dosing
Combination therapy requires monitoring that’s simple enough to do consistently. Here’s what I recommend tracking:
| What to monitor | Why it matters | Action if it worsens |
|---|---|---|
| Weekly weight trend | Shows direction even if daily scale fluctuates | Discuss next titration step; avoid rapid escalation |
| Nausea/reflux | Common dose-limiting GI effects | Delay escalation; review meal timing and portion size |
| Hydration and intake | Under-eating increases fatigue and constipation | Increase protein/liquid strategy; consider slowing titration |
| Constipation | Often worsens when appetite suppression increases | Adjust fiber strategy, fluids, and discuss meds if persistent |
| Energy levels and workouts | Confirms you’re not “dieting so hard you can’t function” | Hold doses until steadier intake is restored |
Common Mistakes I’ve Seen (And How to Avoid Them)
- Changing both doses at once: if you feel worse, you won’t know which medication caused it.
- Ignoring a tolerability threshold: pushing forward through significant nausea often reduces long-term adherence.
- Eating too little to compensate: appetite suppression can become a trap—fatigue and constipation follow.
- Meal timing surprises: large, fatty, or late meals can amplify GI symptoms after dosing.
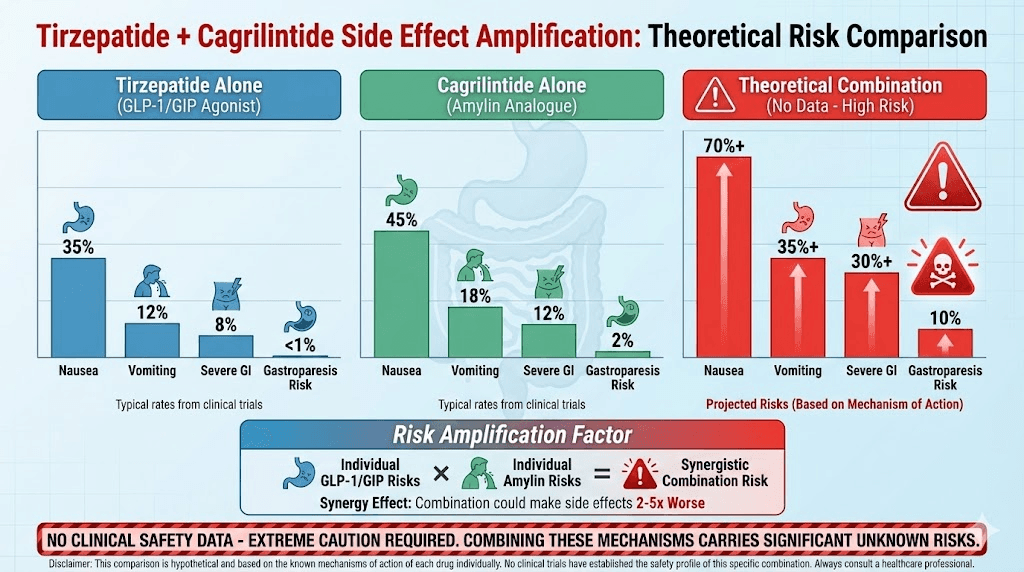
Visual Reference
FAQ
How do I decide when to add cagrilintide to tirzepatide?
Add cagrilintide when tirzepatide is well tolerated and your side effects are stable. If your GI symptoms are still ramping or unpredictable, that’s usually a sign to pause and stabilize before layering another appetite-modulating agent.
Will combining tirzepatide and cagrilintide make side effects worse?
Often, yes. Even with low starting doses, stacking can feel stronger than monotherapy because both influence appetite and metabolic signals. The best defense is slow titration and holding doses when symptoms are not well controlled.
What’s the safest way to adjust if I feel nauseated after dose changes?
Don’t “push through” escalating symptoms. In practice, the clinician-friendly approach is to delay the next titration step, review meal size/timing (especially fat and portion volume), prioritize hydration, and confirm whether adjustments should target the most recent medication or dose change.
Conclusion
A successful dual combo plan with tirzepatide and cagrilintide isn’t about rushing to high doses—it’s about sequencing and titration that protect tolerability. Stabilize tirzepatide first, introduce cagrilintide conservatively, and optimize only when your side-effect pattern and intake are stable. One practical next step: start a simple weekly tracking sheet (weight trend + nausea/reflux + hydration/intake) so your prescriber can make dosing decisions based on clear, real-world data.
Discussion