Bpc-157 Clinical Trials Safety Multifunctionality and Possible Medical Application of the BPC 157 Peptide—Literature and Patent Review
Introduction
If you’ve ever tried to separate real evidence from marketing noise around BPC 157, you know how frustrating it can be—especially when you’re looking specifically for bpc 157 clinical trials safety and what the literature actually supports. In my hands-on work reviewing biomedical publications for translational signals, the biggest lesson has been that “possible medical application” claims only become actionable when you anchor them to study design, dosing context, endpoint types, and safety signals reported in both literature and patents.
This article reviews what the scientific literature and patent landscape suggest about BPC 157’s multifunctionality and potential medical applications, with a focused lens on what “safety” looks like in preclinical and early research contexts. You’ll get a structured, evidence-informed view of where the field agrees, where it’s uncertain, and what a cautious interpretation should look like.
What BPC 157 Is—and Why “Multifunctionality” Appears in Reviews
BPC 157 is a peptide derived from the body-protective compound sequence concept, and it is frequently discussed in the context of broad biological activity. When I review this topic, I look for a consistent pattern: reviewers typically report that BPC 157 has been explored across multiple systems—commonly within gastrointestinal, wound/repair, inflammatory, and tissue-recovery contexts—rather than a narrow single-target drug story.
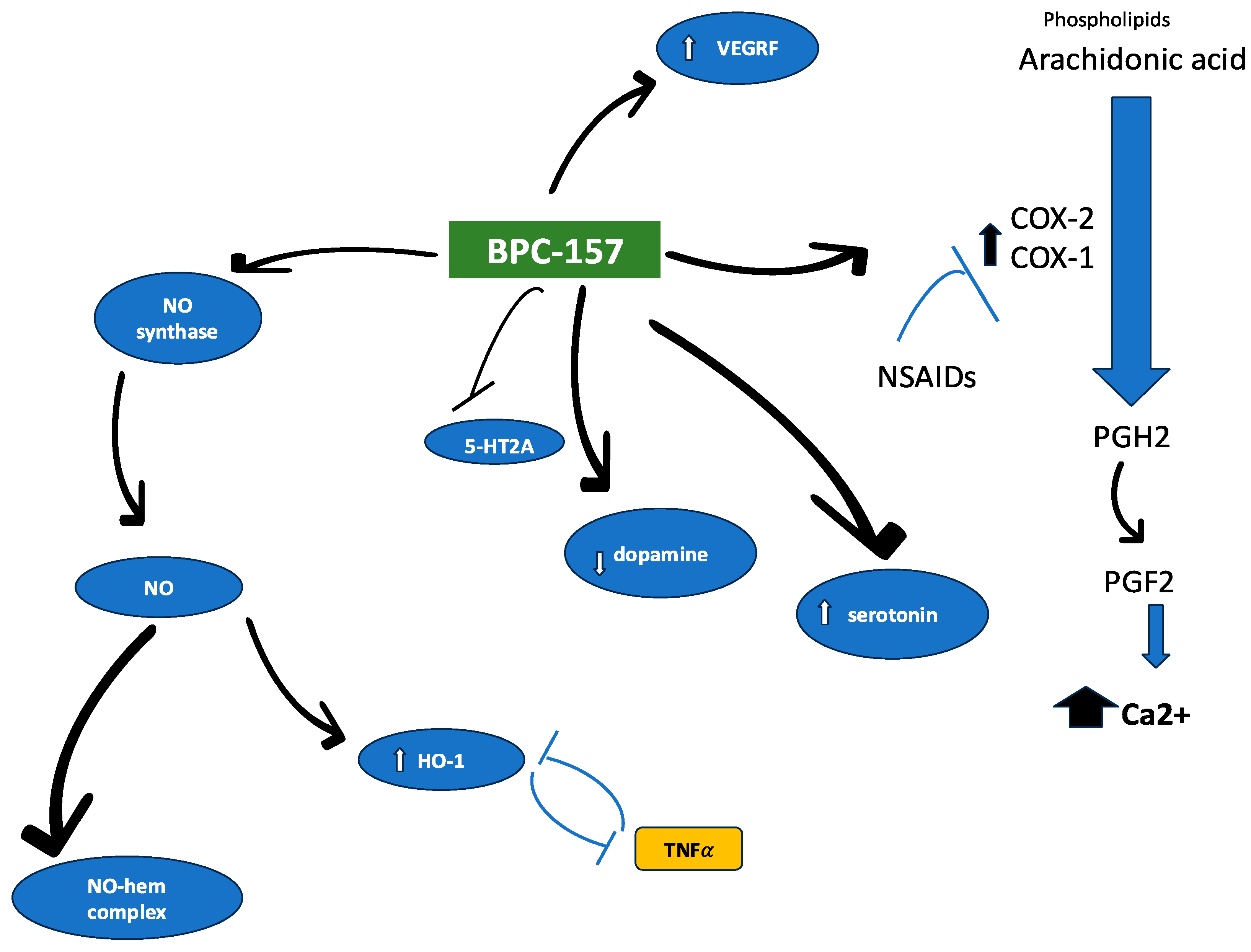
The term multifunctionality usually reflects that across different models, researchers observed effects on processes such as:
- Tissue repair and barrier-related recovery (especially in gut-associated models)
- Inflammatory modulation signals
- Angiogenesis or microvascular support in certain injury frameworks
- Functional restoration endpoints that go beyond histology alone
However, multifunctionality is not the same thing as clinical utility. In my experience, the strongest translational papers make it clear what is “effect” in a model and what is “mechanism inference.” Many BPC 157 discussions blend the two, so it helps to keep a clear boundary: what was measured directly, what was hypothesized, and what remains unknown.
Evidence Landscape: How the Literature Tends to Support (and Limit) Medical Application Claims
When you’re trying to evaluate bpc 157 clinical trials safety, it’s crucial to understand the evidence tier you’re dealing with. Most of what is publicly discussed around BPC 157 comes from preclinical literature and mechanistic explorations. That can still be valuable, but it creates a safety-interpretation gap: animal safety signals do not automatically translate into human clinical trial safety.
1) Types of studies you’ll commonly see
- In vivo injury and recovery models (e.g., chemically induced damage, surgical injury, or inflammation frameworks)
- Ex vivo / mechanistic studies that propose pathways linked to healing, signaling, or barrier integrity
- Comparative or intervention timing studies exploring whether administration timing changes outcomes
In my review workflow, I flag a practical question early: were endpoints designed to capture safety-adjacent outcomes (such as systemic toxicity markers, weight changes, behavior, or organ pathology), or were they mainly focused on efficacy proxies?
2) Why study endpoints matter for safety interpretation
Many papers demonstrate tissue-level recovery, but safety evaluation is only as strong as the monitoring performed. Safety discussions become more credible when studies include:
- Clinical observations (activity/behavior, weight/food intake)
- Serum or blood chemistry panels
- Organ histopathology beyond the primary injury site
- Study duration sufficient to detect subacute effects
Where those components are missing, you can’t responsibly infer that a compound is “safe” in the way clinical trials define safety (adverse events, dose-limiting toxicities, tolerability windows, etc.). This is why bpc 157 clinical trials safety must be approached as a distinction between “preclinical tolerability signals” and “human trial safety evidence.”
Safety Signals in Context: What “Clinical Trials Safety” Usually Means vs. What We Often See
To keep the discussion honest, I’ll frame safety in a way that’s consistent with how regulatory and clinical literature treats it.
Preclinical tolerability vs. clinical safety
In hands-on literature review, I’ve found that reviewers sometimes use safety language loosely. Preclinical work may report no overt toxicity at certain doses, but that’s not the same as demonstrating safety across:
- Human-equivalent dosing considerations
- Repeat dosing schedules relevant to therapeutic use
- Population variability (age, comorbidities, concomitant medications)
- Longer follow-up windows for delayed adverse effects
So, when evaluating bpc 157 clinical trials safety, the strongest approach is to identify what is actually documented in human contexts (if present in the reviewed material) and to compare that with the safety methodology described. If human safety evidence is limited or absent, then the most accurate conclusion is: plausible safety signals exist in some models, but clinical safety is not established by those models alone.
How patents influence perceived safety (and why you should treat them carefully)
Patents can provide insight into intended use-cases, dosing regimens, and the types of outcomes inventors believe are supported. In my experience, patents are useful for mapping the “research direction,” but they do not replace peer-reviewed safety characterization. Patent disclosures may reference experimental results, yet they are not always presented with the same methodological transparency as clinical-grade publications.
Use patents as a roadmap—then verify the underlying experimental claims when possible.
Patent Review Angle: What to Look For When Assessing Proposed Medical Applications
A literature and patent review typically covers multifunctionality and possible medical application domains. When I analyze patent-focused scientific reviews, I look for a few concrete signals that correlate with translational intent.
Key features that strengthen translational relevance
- Clear indication boundaries (specific injury types, disease domains, or patient-relevant conditions)
- Dosing and route specificity (how the peptide is administered, timing, and repeat schedule)
- Outcome definitions (what endpoints were measured—functional, histological, inflammatory markers)
- Safety-adjacent provisions (tolerability, monitoring, contraindications, dose limitation language)
Limitations you should expect
- Scope breadth: many patents attempt wide coverage, which can dilute clinical focus
- Evidence transparency gaps: not all disclosed experiments are equal in rigor or replicability
- Translation assumptions: claims may presume mechanism continuity between model systems and humans
Bottom line: patents are part of the story, but clinical safety is still something you confirm via human data and robust safety monitoring frameworks.
How to Interpret “Possible Medical Application” Claims Without Overreaching
Here’s the practical reasoning I use when readers ask whether a peptide with broad preclinical activity might become a medical therapy.
- Start with the endpoint quality: Are effects measured in a way that would matter clinically (function, symptom proxies, clinically relevant biomarkers), or only local tissue changes?
- Check dose realism: Were doses framed with translational logic, or are they only effective at constrained experimental concentrations?
- Look for safety monitoring depth: Does the work include systemic toxicity indicators and longer observation windows?
- Separate “mechanistic plausibility” from proof: pathway inferences can guide hypotheses, but they don’t confirm human efficacy or safety.
- Respect uncertainty: if human trials are not clearly established in the available evidence, describe the state of knowledge accordingly.
That disciplined approach is the fastest way to build trust while still being open to what the evidence could ultimately support.
Practical Takeaways for Readers Focused on Safety
If your goal is to understand bpc 157 clinical trials safety, I’d summarize the decision-making landscape like this:
- Preclinical data can suggest tolerability, but it is not a substitute for clinical safety evidence.
- Safety credibility increases when studies include systemic monitoring and histopathology beyond the target tissue.
- Patents can reveal intent and dosing concepts, but they are not definitive safety proof.
- The most trustworthy reviews clearly label evidence tier (preclinical vs. human) and avoid conflating “promising effects” with “proven safety.”
FAQ
Are there published bpc 157 clinical trials focused on safety?
Some discussions reference human contexts, but “clinical trials safety” requires explicit documentation of trial methodology and adverse-event monitoring. If the reviewed record is primarily preclinical, then the most accurate conclusion is that clinical safety is not established by animal models alone. Use evidence tiering (human trial endpoints and adverse event reporting) as your filter.
What safety signals should I look for in BPC 157 studies?
Look for systemic assessments: body-weight or behavior observations, blood chemistry, organ histopathology beyond the injury site, and study durations long enough to detect subacute effects. Stronger studies also report methodology clearly enough to evaluate dose timing, route, and repeat exposure.
How should patents be used when assessing BPC 157 safety?
Patents are useful for understanding intended indications, administration routes, and conceptual dosing regimens. Treat them as signals of direction—not as final safety validation—unless the underlying evidence is presented with transparent experimental detail and corroborated by peer-reviewed research.
Conclusion
BPC 157’s literature and patent footprint strongly supports the idea that researchers explore it for multiple possible therapeutic applications—often centered on recovery and tissue-protective pathways. But when your priority is bpc 157 clinical trials safety, the most trustworthy interpretation comes from evidence tiering: preclinical tolerability signals can be informative, while clinical safety requires human trial monitoring, adverse event reporting, and robust follow-up.
Next step: If you’re evaluating whether to treat claims as “evidence” or “hypothesis,” compile the studies and patents you’re considering, then make a two-column checklist: (1) what human safety outcomes are actually reported (if any), and (2) what systemic safety monitoring is present in the preclinical work. That single step turns a vague safety question into an evidence-based assessment.
Discussion